

SAN DIEGO—Cognitive behavioral therapy decreased pain and improved some measures of sleep in a study of patients with Crohn’s disease suffering from insomnia presented at DDW 2025.
Poor sleep is a fact of life for more than half of patients with inflammatory bowel disease, causing fatigue that affects their overall quality of life (Sleep Adv 2022;3[1]:zpac025; JGH Open 2024;8[8]:e70021), noted investigator Jessica K. Salwen-Deremer, PhD, who presented the results at the meeting (presentation 567).
Dr. Salwen-Deremer, an assistant professor and a staff psychologist at Dartmouth Hitchcock Medical Center, in Lebanon, N.H., explained that beyond causing everyday pain and discomfort, such fatigue can have grueling long-term effects on patients with IBD, increasing the probability of flares, hospitalization and the need for surgical intervention (Inflamm Bowel Dis 2020;26[10]:1524-1532).
Laurie Keefer, PhD, a gastropsychologist and clinical health psychologist at the Icahn School of Medicine at Mount Sinai, in New York City, said improving sleep hygiene—such as not looking at screens 30 minutes before bed and waking up and going to sleep at the same time each day—can help, but when a patient’s insomnia is long-lasting, “you really need a much more targeted intervention.”

Cognitive behavioral therapy “can be delivered [quickly] by trained professionals,” Dr. Keefer said, noting that it can be more effective than sleep medications (Ann Intern Med 2016;165[2]:125-133). “It is really incredible in that it also reduces pain intensity and pain interference, ... but [it] has not been studied in IBD, only in other pain populations,” she said.
To evaluate the potential role of cognitive behavioral therapy in the setting of CD and insomnia, Dr. Salwen-Deremer and her co-investigators conducted a pilot study, enrolling patients with acute symptoms of CD and insomnia who were treated at the Dartmouth Hitchcock IBD Center. Of the 41 enrolled patients, 26 completed the study. Approximately 65.4% of the participants were women and 88.5% were white. The median age was 44.5 years.
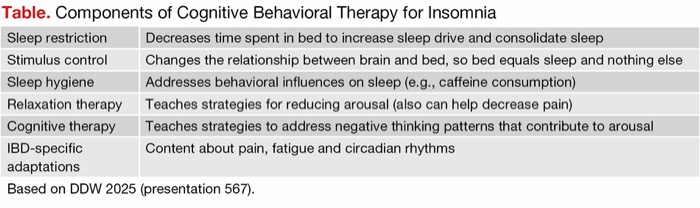
| Table. Components of Cognitive Behavioral Therapy for Insomnia | |
| Sleep restriction | Decreases time spent in bed to increase sleep drive and consolidate sleep |
| Stimulus control | Changes the relationship between brain and bed, so bed equals sleep and nothing else |
| Sleep hygiene | Addresses behavioral influences on sleep (e.g., caffeine consumption) |
| Relaxation therapy | Teaches strategies for reducing arousal (also can help decrease pain) |
| Cognitive therapy | Teaches strategies to address negative thinking patterns that contribute to arousal |
| IBD-specific adaptations | Content about pain, fatigue and circadian rhythms |
| Based on DDW 2025 (presentation 567). | |
The patients completed evaluations, including questionnaires, sleep assessments and a pain tolerance test, and submitted stool and blood samples. They then were randomized to one of two groups: One completed five 45-minute cognitive behavioral therapy sessions that incorporated training on sleep hygiene, relaxation therapy and other strategies (Table); they also had five- to 10-minute telephone calls with therapists between sessions and filled out a daily journal before a reassessment 12 weeks later. A control group, the waitlist group, was reassessed at 12 weeks and then underwent the intervention.
Benefits Related to Insomnia, Disease Severity and Pain
The researchers found that the Insomnia Severity Index score decreased by more than 10 points (P<0.001) in patients who underwent cognitive behavioral therapy, whereas it decreased by less than 1 point in the control group.
The mean Crohn’s Disease Activity Index score (three-item patient-reported outcomes subscale) decreased from 23.87 before cognitive behavioral therapy to 19.88 immediately after treatment and to 17.05 one month after treatment, for an overall symptom reduction of F=4.88 (P=0.01). Pain intensity decreased from 4.04 to 3.14 immediately and to 3.1 one month after treatment (F=4.15; P=0.02), while pain interference decreased from 4.02 to 2.56 immediately and to 2.5 one month after treatment (F=5.05; P=0.01).
Cognitive behavioral therapy did not have a significant effect on rates of sleep continuity throughout the entire night, but it resulted in improvements in the time it took participants to fall asleep and the time spent sporadically awake during the night.
“This is consistent with the literature across other populations,” Dr. Salwen-Deremer said. It improved “slow-wave sleep, our deepest stage of sleep, and the amount of time in that stage of sleep increased with intervention,” she added.
Related Content



Statistically significant improvements also were seen in psychosocial outcomes of fatigue, such as anxiety and depression.
The investigators did not see any benefit of cognitive behavioral therapy on inflammatory markers (C-reactive protein and fecal calprotectin).
Although Dr. Keefer acknowledged some of the standard limitations of the pilot study, such as a predominantly white population and a small sample size, she said the rigor of this study is building a foundation to illustrate the benefits of cognitive behavioral therapy in IBD patients.
“Randomized controlled trials with well-characterized populations of IBD ... looking at both sleep and inflammatory markers [are needed],” she said. “This study is a great example of that and will hopefully lead to the incorporation of [cognitive behavioral therapy] into routine IBD care for those suffering.”
—Karen Fischer
Dr. Keefer reported financial relationships with AbbVie, Ardelyx, J&J, Lilly and Pfizer. She also is an equity owner/ co-founder/advisor for Trellus Health. Dr. Salwen-Deremer reported a financial relationship with Buhlmann Diagnostics.
This article is from the July 2025 print issue.