

Johns Hopkins University School of Medicine
Baltimore, Maryland
An ideal bowel preparation should have many attributes, including the ability to reliably empty the colon in a rapid fashion, without causing any gross or histologic alteration of colonic mucosa, shifts in fluids and electrolytes, or patient discomfort, and it should be relatively inexpensive.
This article discusses quality measures for bowel preparation, as well as various tools to measure the quality of bowel preparation and ways to improve it. This review is meant to provide gastroenterologists and endoscopists with strategies and best practices to get their patients to optimize bowel preparation.
Why Measure the Quality Of Bowel Preparation?
Having reliable measures of the quality of bowel preparation is important, as that quality affects our ability to detect polyps during colonoscopy as well as the cost of colonoscopy. Poor or incomplete visualization of the colon reduces the yield of screening colonoscopies and increases health care costs, due to longer procedure times and aborted procedures. Chokshi et al studied the prevalence of missed adenomas in patients with inadequate bowel preparation for screening colonoscopy and noted that among 133 patients with initially suboptimal bowel preparation, 33.8% had at least 1 adenoma detected on repeat colonoscopy and 18% had high-risk lesions detected.1 Tholey et al showed that excellent bowel preparation resulted in superior detection of sessile serrated polyps and advanced adenomas compared with good preparation.2 Rex et al investigated the impact of bowel preparation on the efficiency and cost of colonoscopy; their cost analysis showed that imperfect bowel preparation results in a 12% increase in costs at university hospitals and a 22% increase in costs at public hospitals.3 They found that aborted examinations and earlier repeat surveillance examinations related to suboptimal bowel preparations increased the costs associated with colonoscopy.
Ways to Measure the Quality Of Bowel Preparation
There are many ways to characterize bowel preparation. The quality can be labeled as excellent, good, fair, or poor; however, the lack of standardized definitions for these labels can cause significant interobserver variability. Bowel preparation quality also can be characterized as adequate versus inadequate based on its ability to allow for detection of polyps greater than 5 mm. Various scoring systems, such as the Boston Bowel Preparation Scale (BBPS) and Ottawa Bowel Preparation Scale (OBPS), have been well validated and have high interobserver and intra-observer reliability.

The BBPS divides the colon into 3 broad regions: right side (cecum and ascending colon), transverse section (transverse colon including the hepatic and splenic flexures), and left side (descending colon, sigmoid colon, and rectum); each region of colon receives a segment score from 0 to 3 based on visual inspection of colon during colonoscopy. These segments are summed for a total BBPS score ranging from 0 (for an unprepared colon) to 9 (for a perfectly clean colon). The BBPS is applied during the withdrawal phase of colonoscopy. If a procedure is aborted due to inadequate preparation, then any nonvisualized proximal segments are assigned a score of 0. The BBPS has been well validated and shown to have high inter- and intra-observer reliability. Also, higher BBPS scores (>5 vs <5) have been associated with higher polyp detection rates (40% vs 24%; P<0.02).4
The OBPS rating for each colon segment is different from the BBPS, such that a higher score is given to each segment for poor preparation and a score also is given for the amount of fluid in the whole colon. The scores of the right, transverse/descending, and sigmoid/rectum and the score for the fluid in the whole colon are added to generate an OBPS score ranging from 14 (very poor) to 0 (excellent).5
In the BBPS, analysis is done during withdrawal, after all the cleaning maneuvers, allowing better assessment of bowel preparation and reflecting an ability to detect polyps; in the OBPS, analysis is done before cleaning attempts by the endoscopist, comparing quality of cleanliness and reflecting efficacy of bowel preparation regimens (Table 1).
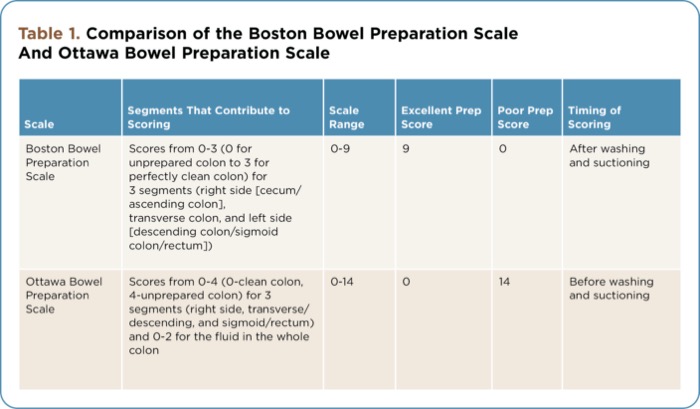
| Table 1. Comparison of the Boston Bowel Preparation Scale And Ottawa Bowel Preparation Scale | |||||
| Scale | Segments That Contribute to Scoring | Scale Range | Excellent Prep Score | Poor Prep Score | Timing of Scoring |
|---|---|---|---|---|---|
| Boston Bowel Preparation Scale | Scores from 0-3 (0 for unprepared colon to 3 for perfectly clean colon) for 3 segments (right side [cecum/ascending colon], transverse colon, and left side [descending colon/sigmoid colon/rectum]) | 0-9 | 9 | 0 | After washing and suctioning |
| Ottawa Bowel Preparation Scale | Scores from 0-4 (0-clean colon, 4-unprepared colon) for 3 segments (right side, transverse/descending, and sigmoid/rectum) and 0-2 for the fluid in the whole colon | 0-14 | 0 | 14 | Before washing and suctioning |
The American Society for Gastrointestinal Endoscopy (ASGE)/American College of Gastroenterology (ACG) Task Force on Quality in Endoscopy published the quality indicators for colonoscopy.6 It sets performance targets of greater than 98% for documenting the quality of preparation in the procedure note and greater than 85% for adequate bowel preparations for outpatient colonoscopy examinations. An adequate bowel preparation allows detection of polyps greater than 5 mm in size; if bowel preparation is not adequate, then the procedure should be repeated within 1 year. If inadequate bowel preparation is noted in more than 15% of colonoscopy examinations at a facility, then it is imperative that the facilty reexamines its bowel preparation protocols, patient education, choice of purgative, and protocols for administering the purgative, with the goal of achieving the performance target.
Improve the Quality of Bowel Preparation
To get perfect bowel preparation in each patient, it is important to identify factors associated with poor bowel preparation and target resources to patients who are at increased risk. Ness et al identified the predictors for inadequate bowel preparation for colonoscopy; these included procedure time, preparation instructions not followed, a history of cirrhosis, inpatient status, constipation as the indication for the procedure, tricyclic antidepressant use, male sex, and a history of stroke or dementia.7 Lebwohl et al studied socioeconomic and other predictors of colonoscopy preparation quality and identified Medicaid insurance and time of colonoscopy after 11 am as factors associated with poor bowel preparation quality.8 Kunnackal et al identified factors affecting the quality of bowel preparation and found that poor health literacy, low functional status, and a high number of daily medications are significant factors predicting inadequate bowel preparation in the tertiary care setting.9 Future quality improvement efforts should target populations with these characteristics to successfully improve rates of adequate bowel preparation.
Another method shown to result in more satisfactory bowel preparation is the use of split-dose preparation. In a randomized controlled trial, Aoun et al compared the efficacy of 2 bowel preparation regimens: a whole dose (4 L) of polyethylene glycol electrolyte solution (PEG) with diet restriction on the night before the procedure versus a split dose (2 L of PEG on the evening before and 2 L on the morning of the procedure) with no diet restriction. Colonic preparation with split-dose PEG provides better colon cleansing than whole-dose preparation (P=0.011), with no significant impact on patient tolerability or side effects.10 Enestvedt et al conducted a meta-analysis of split-dose PEG versus other bowel preparations and found that the pooled odds ratio (OR) for excellent or good bowel preparation quality for split-dose PEG was 3.46 compared with other methods (95% CI, 2.45-4.89; P<0.01); they concluded that split-dose PEG is better than other bowel preparation methods for colonoscopy and suggested that split-dose PEG should be considered the standard for bowel preparation methods.11
Siddiqui et al showed that bowel preparation quality varies inversely with the duration of the interval between the last dose of the bowel preparation agent and the start of colonoscopy, and the quality of bowel preparation decreased as the interval increased between the end of the preparation ingestion and start of the procedure, such that the optimal window was typically 8 hours or less.12 To improve the quality of bowel preparation, ideally one should aim for split dosing, such that half of the preparation is given on the day of the examination started 4 to 5 hours before the procedure and completed at least 2 hours before the procedure (to reduce aspiration risk). For patients who are scheduled for afternoon colonoscopies, the entire preparation can be ingested on the day of the exam.
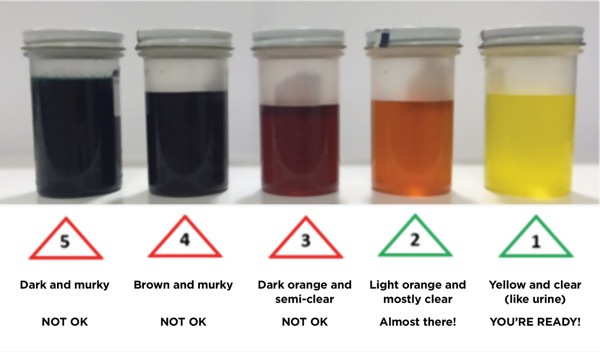
Another way to improve the quality of bowel preparation is by using a tool such as the “Colonoscopy Visual Preparation Card,” which is based on patients’ reported stool color from their last bowel movement, to evaluate the adequacy of their bowel preparation (Figure). This empowers patients to take necessary steps to improve the quality of their bowel preparation. The visual nature of this tool, along with definite written directions, may help allay anxiety and provide confidence to patients about the adequacy of their bowel preparation. This can translate into improvement in the quality of their bowel preparation scores. This tool has been validated in both direct access and outpatient colonoscopy settings.13 The color of the patient’s most recent stool before they arrive for the procedure was significantly associated with adequate bowel preparation (P<0.001); compared with yellow and clear stools, the following stool colors were associated with higher odds of inadequate bowel preparation: light orange and mostly clear (OR, 4.1; P<0.01), dark orange and semi-clear (OR, 14.5; P<0.001), and brown and murky (OR, 18.1; P<0.001).14
Selecting a Bowel Preparation
The common bowel preparations fall under 3 broad categories: 1) PEG solutions, which are high-volume gut lavage solutions; 2) osmotic agents, such as sodium phosphate, magnesium citrate, and the newly approved sodium sulfate, magnesium sulfate, and potassium chloride tablets (Sutab Sebela), which draw extracellular fluid across the bowel wall and into the lumen; and 3) stimulants, such as castor oil, senna, sodium picosulfate, and bisacodyl, which increase smooth muscle activity within the wall of the colon.
The common commercially available bowel preparations are listed in Table 2. The PEG solutions are nonabsorbable, do not cause substantial shifts in fluids and electrolytes, and are relatively safer to use in patients with advanced liver disease, congestive heart failure, and renal failure. The major disadvantages of these PEG solutions are that ingestion of a large amount of solution that can have a poor salty taste is required, leading to poor patient compliance, and these products are contraindicated in patients with allergies to PEG compounds, gastric outlet obstruction, and bowel obstruction. In contrast, the sodium phosphate tablets are more tolerable to patients and do not require ingestion of large volumes, but they can cause renal failure due to hyperphosphatemia (acute phosphate nephropathy), especially in patients who have chronic kidney disease, bowel obstruction, active colitis, or hypovolemia, and/or who take other medications including diuretics, angiotensin-converting enzyme inhibitors, or nonsteroidal anti-inflammatory agents. Sodium phosphate tablets should be avoided in patients with impaired renal function, advanced liver disease, congestive heart failure, and hypercalcemia. They also should be avoided in patients with suspicion of inflammatory bowel disease or chronic diarrhea because they may cause aphthous ulcers in these patients. The sodium picosulfate–based bowel preparations can be considered in patients with a history of bariatric surgery, given the low volume required, but these preparations can be dehydrating and can increase hemoglobin levels; they also should be avoided in older patients due to risks for hyponatremia and orthostatic hypotension.
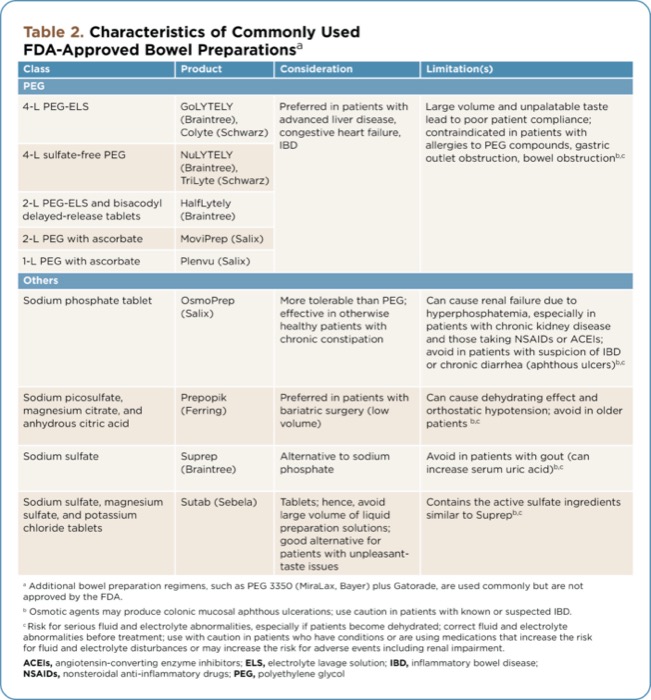
| Table 2. Characteristics of Commonly Used FDA-Approved Bowel Preparations | |||
| Class | Product | Consideration | Limitation(s) |
|---|---|---|---|
| PEG | |||
| 4-L PEG-ELS | GoLYTELY (Braintree), Colyte (Schwarz) | Preferred in patients with advanced liver disease, congestive heart failure, IBD | Large volume and unpalatable taste lead to poor patient compliance; contraindicated in patients with allergies to PEG compounds, gastric outlet obstruction, bowel obstructionb,c |
| 4-L sulfate-free PEG | NuLYTELY (Braintree), TriLyte (Schwarz) | ||
| 2-L PEG-ELS and bisacodyl delayed-release tablets | HalfLytely (Braintree) | ||
| 2-L PEG with ascorbate | MoviPrep (Salix) | ||
| 1-L PEG with ascorbate | Plenvu (Salix) | ||
| Others | |||
| Sodium phosphate tablet | OsmoPrep (Salix) | More tolerable than PEG; effective in otherwise healthy patients with chronic constipation | Can cause renal failure due to hyperphosphatemia, especially in patients with chronic kidney disease and those taking NSAIDs or ACEIs; avoid in patients with suspicion of IBD or chronic diarrhea (aphthous ulcers)b,c |
| Sodium picosulfate, magnesium citrate, and anhydrous citric acid | Prepopik (Ferring) | Preferred in patients with bariatric surgery (low volume) | Can cause dehydrating effect and orthostatic hypotension; avoid in older patients b,c |
| Sodium sulfate | Suprep (Braintree) | Alternative to sodium phosphate | Avoid in patients with gout (can increase serum uric acid)b,c |
| Sodium sulfate, magnesium sulfate, and potassium chloride tablets | Sutab (Sebela) | Tablets; hence, avoid large volume of liquid preparation solutions; good alternative for patients with unpleasant-taste issues | Contains the active sulfate ingredients similar to Suprepb,c |
a Additional bowel preparation regimens, such as PEG 3350 (MiraLax, Bayer) plus Gatorade, are used commonly but are not approved by the FDA. b Osmotic agents may produce colonic mucosal aphthous ulcerations; use caution in patients with known or suspected IBD. c Risk for serious fluid and electrolyte abnormalities, especially if patients become dehydrated; correct fluid and electrolyte abnormalities before treatment; use with caution in patients who have conditions or are using medications that increase the risk for fluid and electrolyte disturbances or may increase the risk for adverse events including renal impairment. ACEIs, angiotensin-converting enzyme inhibitors; ELS, electrolyte lavage solution; IBD, inflammatory bowel disease; NSAIDs, nonsteroidal anti-inflammatory drugs; PEG, polyethylene glycol | |||
Conclusion
It is important to focus on the quality of bowel preparation to get a perfect bowel preparation in every patient because it significantly affects the ability to detect polyps and the costs associated with colonoscopy. Bowel preparation quality should be recorded for every colonoscopy, preferably using a validated scale. The choice of bowel preparation agent needs to be individualized to each patient and should be based on a patient’s age, comorbid conditions, and personal preference.
References
- Chokshi RV, Hovis CE, Hollander T, et al. Prevalence of missed adenomas in patients within adequate bowel preparation on screening colonoscopy. Gastrointest Endosc. 2012;75(6):1197-1203.
- Tholey DM, Shelton CE, Francis G, et al. Adenoma detection in excellent versus good bowel preparation for colonoscopy. J Clin Gastroenterol. 2015;49(4):313-319.
- Rex DK, Imperial TF, Latinovich DR, et al. Impact of bowel preparation on efficiency and cost of colonoscopy. Am J Gastroenterol. 2002;97(7):1696-1700.
- Calderwood AH, Jacobson BC. Comprehensive validation of the Boston Bowel Preparation Scale. Gastrointest Endosc. 2010;72(4):686-692.
- Rostom A, Jolicoeur E. Validation of a new scale for the assessment of bowel preparation quality. Gastrointest Endosc. 2004;59(4):482-486.
- Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc. 2015;81(1):31-53.
- Ness RM, Manam R, Hoen H, et al. Predictors of inadequate bowel preparation for colonoscopy. Am J Gastroenterol. 2001;96(6):1797-1802.
- Lebwohl B, Wang TC, Neugut AI. Socioeconomic and other predictors of colonoscopy preparation quality. Dig Dis Sci. 2010;55(7):2014-2020.
- Kunnackal J, Thuluvath A, Carrier H, et al. Improving the quality of bowel preparation for colonoscopy: populations to target in an urban tertiary care setting. Gastroenterology. 2018;1549(6 suppl 1):S-142-S-143.
- Aoun E, Abdul-Baki H, Azar C, et al. A randomized single-blind trial of split-dose PEG-electrolyte solution without dietary restriction compared with whole dose PEG-electrolyte solution with dietary restriction for colonoscopy preparation. Gastrointest Endosc. 2005;62(2):213-218.
- Enestvedt BK, Tofani C, Laine LA, et al. 4-Liter split-dose polyethylene glycol is superior to other bowel preparations, based on systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2012;10(11):1225-1231.
- Siddiqui AA, Yang K, Spechler SJ, et al. Duration of the interval between the completion of bowel preparation and the start of colonoscopy predicts bowel-preparation quality. Gastrointest Endosc. 2009;69(3 pt 2):700-706.
- Gupta E, Kunnackal J, Linda L. A novel tool “colonoscopy preparation card” using patient reported stool color to improve success of direct access endoscopy. Gastroenterology. 2018;154(6 suppl 1):S-891.
- John GK, Thuluvath AJ, Gupta E, et al. Patient-reported stool color and perception of bowel preparation predicts success of outpatient bowel preparation in an urban tertiary care setting. Gastroenterology. 2018;155(1):e40-e41.
Dr Gupta reported no relevant financial disclosures.
Copyright © 2021 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Bowel Preparation Quality: How to Get Perfect Bowel Preparation for Every Patient
Bowel Preparation Quality: How to Get Perfect Bowel Preparation for Every Patient