

VANCOUVER, B.C.—Three years after the Hospital Price Transparency Rule was implemented by the Centers for Medicare & Medicaid Services, a large proportion of hospitals are not complying when it comes to gastrointestinal services, according to two studies presented at the 2023 annual meeting of the American College of Gastroenterology.
When institutions do list their prices, they are often hard to find, and the wide variety of charges are frequently listed in a format that is “not patient-friendly,” according to investigator Kevin Brittan, MD, an internal medicine resident at the University of Nebraska Medical Center, in Omaha.
Two independent groups of investigators looked at compliance with the price transparency rule for a list of specific GI procedures, such as colonoscopy and liver biopsy. Many of the procedures are elective, so a patient might reasonably want to compare pricing when seeking such a procedures. All hospitals are expected to be in compliance with the rule and report prices for these and other procedures as of Jan. 1, 2021.
However, in one study, Dr. Brittan and his co-investigators found that only two of 25 hospitals surveyed (8%) reported costs for all eight procedures evaluated (abstract P4083). In the other study, from Howard University researchers, 14 of 30 hospitals (47%) provided some costs for four procedures, but only 10 (30%) provided cost information for all of them (abstract P4091).

Investigator Kovid Bhayana, MD, MBA, an internal medicine resident at Howard University, in Washington, D.C., also found “extreme variance” between institutions in the costs cited, raising the question of whether the reported data are even reliable. “There was a 51-fold difference found in the price for an upper endoscopy and a greater than 80-fold difference for a colonoscopy,” Dr. Bhayana reported. Self-pay colonoscopy prices, for example, ranged from $440 to more than $36,000.
A Public Chargemaster
The rule requires every hospital to maintain a charge description manager, or chargemaster, and make it available for online access. The chargemaster should list the costs for common procedures, with stratifications for cash prices for self-pay and minimum and maximum charges a hospital has negotiated with third-party payors. However, although the rule has been in place for several years, this information is mostly unavailable, hard to find, or provided in ways likely to be confusing to a consumer, according to Drs. Brittan and Bhayana.
The 25 hospitals included in the analysis by Dr. Brittan and and his team were top-rated hospitals overall or hospitals with top-rated gastroenterology interventional programs. They sought to identify the median self-pay prices at these hospitals for abdominal ultrasound, CT of the abdomen with contrast, MRI scan of the abdomen with contrast, liver biopsy, and the pathology costs for specimens collected by upper endoscopy, colonoscopy or liver biopsy.
NewYork-Presbyterian Hospital, Memorial Sloan Kettering Cancer Center and Mayo Clinic (Rochester, Minn.) all listed a price of more than $1,000 for an upper endoscopy. In contrast, NYU Langone Hospital, Mount Sinai Hospital and Rush University Medical Center listed a cost of less than $500 for the same procedure. The listed cost of a liver biopsy approached $12,000 at the University of Pittsburgh Medical Center and NewYork-Presbyterian, but was listed as less than $1,500 at the University of Southern California’s Keck Medical Center and NYU Langone, Dr. Brittan reported. The same kind of spread was observed for most other costs they evaluated.
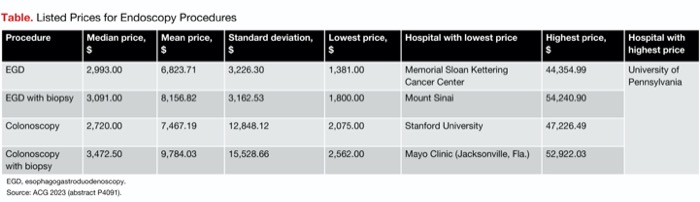
Dr. Bhayana’s team found similar variation (Table). For a diagnostic colonoscopy, the University of Pennsylvania listed a price of $47,266.49. This was the highest price among the 30 hospitals they surveyed. The lowest was $2,075 at Stanford University. The mean price for all hospitals was $7,467.19. “The standard deviation was $12,848.12, which is greater than the mean price,” he noted.
| Table. Listed Prices for Endoscopy Procedures | |||||||
| Procedure | Median price, $ | Mean price, $ | Standard deviation, $ | Lowest price, $ | Hospital with lowest price | Highest price, $ | Hospital with highest price |
|---|---|---|---|---|---|---|---|
| EGD | 2,993.00 | 6,823.71 | 3,226.30 | 1,381.00 | Memorial Sloan Kettering Cancer Center | 44,354.99 | University of Pennsylvania |
| EGD with biopsy | 3,091.00 | 8,156.82 | 3,162.53 | 1,800.00 | Mount Sinai | 54,240.90 | |
| Colonoscopy | 2,720.00 | 7,467.19 | 12,848.12 | 2,075.00 | Stanford University | 47,226.49 | |
| Colonoscopy with biopsy | 3,472.50 | 9,784.03 | 15,528.66 | 2,562.00 | Mayo Clinic (Jacksonville, Fla.) | 52,922.03 | |
| EGD, esophagogastroduodenoscopy. Source: ACG 2023 (abstract P4091). | |||||||
Meaningful Price Comparisons Needed
For Dr. Brittan, the large discrepancies between prices led him to speculate that the law has not spurred a meaningful effort to provide price transparency and, therefore, price comparisons. “Significant outliers were found in multiple procedures, but these outliers were not the same institution with repeat occurrences,” he reported. “Therefore, we suspect the degree of variation in prices demonstrated was not secondary to a few hospitals with high prices—rather, variation was present systematically.”
Approximately 11 million colonoscopies and 6.1 million upper endoscopies performed each year in the United States, Dr. Brittan said. He calculated that the price differences would equate to billions of dollars if procedures were performed at top centers offering the lowest prices relative to top centers asking the highest prices.
The findings indicate that the requirement for price transparency “needs more teeth,” Dr. Bhayana told Gastroenterology & Endoscopy News. Given the likelihood that some institutions are not inclined to reveal the specifics of deals they have made with third-party payors, the data he presented suggest that there should be some penalty or other method of reinforcement when centers are not in compliance.
“To remedy the situation, I think meaningful punishments for those hospitals that are not compliant would be necessary,” Dr. Bhayana said. In addition, he advocated for a uniform reporting format, noting that if hospitals filled in comparable costs in the same format, it would create better apples-to-apples comparisons.
However, Dr. Brittan noted that even these solutions may be too simplistic. “Unfortunately, I do not think there are any clear-cut fixes to the current issue. At this time, penalties for noncompliance do exist, but we cannot be certain of their enforcement as this is not clearly reported. Although a uniform format that would allow apples-to-apples comparisons could be beneficial, medicine is not one-size-fits-all.
“Moreover, we cannot be certain of uniformity of what is included in these cost estimates .... Some may include anesthesia and pathology fees, while others may not,” he told Gastroenterology & Endoscopy News. “These studies demonstrate the desire for further transparency, but do not identify the underlying reasons why we have not achieved the previous set goals.”
A Transparent Future for Patients
So far, patients have been on their own, according to Dr. Bhayana. Even though many physicians are sympathetic to the struggle patients face with healthcare costs, patients typically must obtain and interpret insurance coverage on their own, he said, adding, “I do think that physician support for transparency policies would be beneficial.” Dr. Brittan agreed, saying, “I suspect that next steps forward are continued advocacy for patients to promote greater transparency. This can occur both at an institutional and nationwide level.”
Dr. Bhayana speculated that true cost transparency is probably years away and might require legal action. “There have already been major lawsuits that [advocates for] price transparency won, but I suspect more legal battles are ahead before a transparent healthcare pricing landscape takes form.”
No matter what the path forward, the researchers stated that the Hospital Price Transparency Rule is just the first step. “Although these studies show there is much to be desired, I would not deem cost transparencies law a failure,” Dr. Brittan said. “It was a first step in promoting transparency for patients going forward. I believe further improvements are something we can strive for within the U.S.”
—Ted Bosworth
Drs. Bhayana and Brittan reported no relevant financial disclosures.



This article is from the March 2024 print issue.