


VANCOUVER, B.C.—Over the past few decades, the demographics, location and stage of colorectal cancer at diagnosis have shifted, resulting in new patterns of disease presentation that clinicians should be aware of and that should prompt research to understand the risk factors driving this evolving epidemiology.
In a presentation at the 2023 annual meeting of the American College of Gastroenterology, Folasade May, MD, PhD, MPhil, an associate professor of medicine at the David Geffen School of Medicine at UCLA and the director of the Melvin and Bren Simon Gastroenterology Quality Improvement Program at UCLA Health, in Los Angeles, gave a presentation on four major shifts in the epidemiology of CRC and their implications.
Earlier Age of Onset
Although overall CRC incidence and mortality have been decreasing in the past few decades for people older than 65 years of age, Dr. May highlighted the opposite trend that is occurring among those under 50. She cited data from the Global Health Data Exchange showing that the incidence rate of CRC among those born in the mid- to late 1990s is nearly five times that of those born in the mid- to late 1950s. This has contributed to early-onset CRC (EOCRC) making up a larger proportion of all CRC cases in recent years relative to previous decades. This trend also was reported in a recent study using data from CDC Wonder (Gastro Hep Advances 2024 Jan 19. doi:10.1016/j.gastha.2024.01.004) (see sidebar).
The trend toward EOCRC has not just been seen in the United States. “We’re seeing it globally, throughout regions of East Asia, Europe and Central Asia, Latin America, and the Middle East and North Africa,” Dr. May said. The global nature of this EOCRC shift and the fact that the change has come about relatively quickly point to potential drivers such environmental factors, as opposed to purely genetic factors, according to Dr. May. Thus, “we think it is likely a combination of what we call the exposome, which is your body of lifetime exposures, [as well as] possibly genetic factors, and in addition, somatic alterations,” that is influencing the risk for EOCRC, Dr. May said.

Notable environmental risk factors that are believed to confer significant risk and warrant further study include diet, alcohol and tobacco use, physical activity levels, and very early-life exposures, such as maternal obesity during pregnancy, birth by cesarean delivery, breastfeeding and exposure to antibiotics in childhood. The level of evidence behind each exposure varies, and, particularly for breastfeeding, additional data are needed to understand the strength and direction of the exposure’s association with CRC. Additional factors associated with EOCRC are included in the Table.
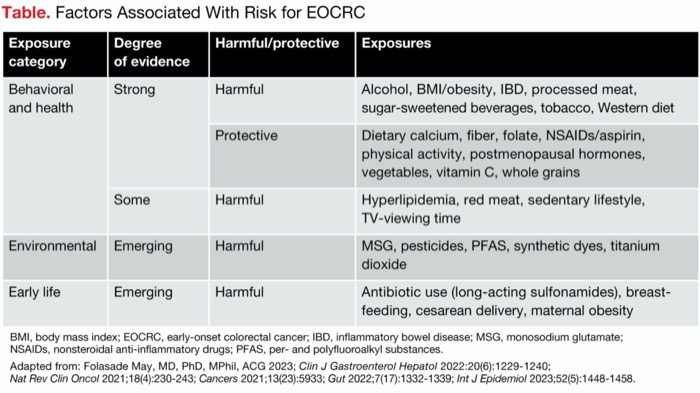
| Table. Factors Associated With Risk for EOCRC | |||
| Exposure category | Degree of evidence | Harmful/protective | Exposures |
|---|---|---|---|
| Behavioral and health | Strong | Harmful | Alcohol, BMI/obesity, IBD, processed meat, sugar-sweetened beverages, tobacco, Western diet |
| Protective | Dietary calcium, fiber, folate, NSAIDs/aspirin, physical activity, postmenopausal hormones, vegetables, vitamin C, whole grains | ||
| Some | Harmful | Hyperlipidemia, red meat, sedentary lifestyle, TV-viewing time | |
| Environmental | Emerging | Harmful | MSG, pesticides, PFAS, synthetic dyes, titanium dioxide |
| Early life | Emerging | Harmful | Antibiotic use (long-acting sulfonamides), breastfeeding, cesarean delivery, maternal obesity |
| BMI, body mass index; EOCRC, early-onset colorectal cancer; IBD, inflammatory bowel disease; MSG, monosodium glutamate; NSAIDs, nonsteroidal anti-inflammatory drugs; PFAS, per- and polyfluoroalkyl substances. Adapted from: Folasade May, MD, PhD, MPhil, ACG 2023; Clin J Gastroenterol Hepatol 2022:20(6):1229-1240; Nat Rev Clin Oncol 2021;18(4):230-243; Cancers 2021;13(23):5933; Gut 2022;7(17):1332-1339; Int J Epidemiol 2023;52(5):1448-1458. | |||
Location of Disease
The second major evolution in CRC epidemiology that Dr. May highlighted is an increasing proportion of disease in the distal colon and rectum relative to the proximal colon. She pointed out that some epidemiological studies have shown that “distal colorectal cancers are associated with high intake of red meat, processed meat and lifetime alcohol exposures” and that there is some evidence of an association between “tobacco use and risk for rectal cancer” (BMJ Open Gastroenterol 2019;6[1]:e000313; Clin Gastroenterol Hepatol 2019;17[7]:1323-1331; Lancet Gastroenterol Hepatol 2022;7[3]:262-274; Nat Rev Gastroenterol Hepatol 2020;17[6]:352-364). However, the data are limited, particularly in terms of their ability to enhance the understanding of how these risk factors act to influence tumor location. There is also ongoing research into whether “embryonic origins of the rectum, infectious agents, pro-inflammatory states or the microbiome are related to where tumors occur and how they progress,” Dr. May said.
Stage at Diagnosis
The third trend is toward advanced stage at diagnosis, particularly seen since 2006 (CA Cancer J Clin 2023;73[1]:17-48). This shift, Dr. May pointed out, “is highly correlated with the shift to left-sided disease and also early-onset” disease and “is driven by individuals who are aged 20 to 49.” In the case of early-onset cancer, Dr. May said, “there is a lot of symptom negligence, either from patients or providers who do not notice symptoms or link them to cancer risk, and, because of that, those individuals are more likely to present with advanced-stage disease.” To Dr. May, the increase in the proportion of CRC cases diagnosed at an advanced stage is “very concerning, because as the disease becomes more advanced, the cure rates are much lower.”
Changing Demographics
Significant shifts in CRC epidemiology also have occurred across racial and ethnic demographic groups, Dr. May noted. American Indian/Alaska Native and Black/African American patients have the two highest incidences of CRC (Colorectal Cancer Facts & Figures 2023-2025, cancer.org/research/cancer-facts-statistics/colorectal-cancer-facts-figures.html). Over the past few decades, the incidence disparity between Black/African American and white individuals has decreased while the incidence disparity between American Indian/Alaska Native and white individuals has increased.
Scoping CRC Incidence Trends
Colorectal cancer incidence is decreasing, but a closer look at trends by age, sex, and race and ethnicity uncovers important patterns that may lead to reconsideration of how to best employ screening and other preventive interventions.
A team of researchers across the United States analyzed data from the CDC’s Wide-Ranging Online Data for Epidemiologic Research (WONDER), a resource that comprehensively collects national cancer diagnoses, to assess trends in CRC incidence between 2000 and 2019, both overall and among key demographic subgroups (Gastro Hep Advances 2024. doi:10.1016/j.gastha.2024.01.004).

During the 20-year period, CRC cases fell for both women and men. Although more cases are diagnosed in men, the average annual decrease in cases is slightly greater for men than women (average annual percent change [AAPC], –2.6; 95% CI, –2.8 to –2.4 vs. –2.3; 95% CI, –2.4 to –2.1).
These findings suggest that “advancements in screening methodologies played a pivotal role in the observed decline in CRC incidence among older individuals,” according to the researchers, led by senior investigator Aasma Shaukat, MD, MPH, a professor in the Departments of Medicine and Population Health at NYU Grossman School of Medicine, in New York City.
A reduction in CRC incidence also was seen for all of the racial and ethnic groups analyzed, but to different extents. Non-Hispanic Black/African Americans had the largest decrease (AAPC, –2.5; 95% CI, –2.7 to –2.3), although they remained the group with the highest incidence throughout the study period. The AAPC was –2.4% (95% CI, –2.6% to –2.2%) for non-Hispanic whites, –2.3% (95% CI, –2.4% to –2.1%) for non-Hispanic Asians, –1.9% (95% CI, –2.1% to –1.8%) for non-Hispanic American Indian/Alaska Natives, and –1.6% (95% CI, –1.8% to –1.3%) for Hispanics.
Among young adults (<45 years old), CRC increased between 2000 and 2019 by 2.4% per year, on average (95% CI, 2.2%-2.7%). Although CRC cases in younger adults made up just 5.4% of all CRC cases in the study period, the trend is concerning, particularly because it is opposite to that seen in older adults, the investigators noted.
This increase was seen in men and women under 45 years old, but it was greater in women (2.6% [95% CI, 2.2%-2.9%] vs. 2.3% [95% CI, 2.0%-2.6%]). The increase was also seen in younger adult members of each race and ethnic group analyzed. The young adult groups with the largest and smallest increases were whites (AAPC, 2.8%; 95% CI, 2.5%-3.0%) and Black/African Americans (AAPC, 0.9%; 95% CI, 0.7%-1.1%), respectively.
Noting that this is the first study to “objectively analyze the changing trends in incidence among different racial/ethnic groups and stratify them into age groups to better explore reasons behind these trends,” the researchers noted that their findings “can assist clinicians, patients, and policymakers in understanding national trends of decreasing CRC incidence with a simultaneous increase in younger individuals” while “underscoring the need to prioritize efforts in screening and other interventions.”
Although American Indian/Alaska Native and Black/African American patients also have the highest incidences of EOCRC, the rate of increase in early-onset disease varies across racial and ethnic groups, “with the highest impact in white and Latino individuals,” Dr. May pointed out. “This is important because the racial and ethnic profile of the United States has changed dramatically over time,” becoming more diverse. “The higher rate of rise in early-onset colorectal cancer in Latino individuals will become even more concerning as Latinos become a larger subset of the population.”
What’s Driving These Shifts?
To better understand the various risk factors and how they are driving these epidemiological shifts, Dr. May suggested several avenues for future research. For one, “there is a great need for large prospective longitudinal cohort studies, particularly with biospecimens, [which] would help us to understand the associations between novel genetic and [environmental] exposures and CRC risk throughout a lifetime,” including key risk periods.
In addition, to better understand environmental exposures, Dr. May recommended “doing cohort studies where we look at birth cohorts” as opposed to just age at diagnosis, “because I think that would give us a lot more information about what birth cohorts are exposed to over time and how that might be related to CRC risk.”
With the different CRC and EOCRC trends seen in different demographic groups, “not only do we need to look at data and trends and exposures by race/ethnicity, but we need to disaggregate our racial and ethnic groups,” Dr. May said. Often, we lump many racial/ethnic subgroups into one group and assume that they “have the same risk [when] we’ll get more clues about what is causing these trends if we disaggregate these groups into their separate populations or origin,” she added.
“As we wait for the science that will tell us about what is causing these epidemiological shifts,” Dr. May recommends focusing on three “things that we can do now and should be doing now.” Her “big three in CRC” are: “1) Be aware of family history, and screen early if there is one; 2) screen everyone else beginning at exactly age 45; and 3) always act on symptoms.” She said, “when patients and doctors do these three things, we will find the majority of cases in time for a high likelihood of cure.”
Underscoring the significance of these epidemiological trends, Seth A. Gross, MD, FACG, FASGE, AGAF, the clinical chief of the Division of Gastroenterology and Hepatology at NYU Langone Health, in New York City, agreed that appropriate screening is a crucial way to help address them. “Average-risk screening starts at age 45, so it is important that the 45- to 50-year-old patient population is aware of this change. Gastroenterologists must educate their referring physicians and patients about the new CRC screening guidelines” to get more of these patients screened.
—Natasha Albaneze, MPH
Dr. Gross is a member of the Gastroenterology & Endoscopy News editorial board.



This article is from the March 2024 print issue.