


Bariatric surgery dramatically decreases the conversion from prediabetes to type 2 diabetes mellitus, according to a study presented at the 2024 annual meeting of the American Society for Metabolic and Bariatric Surgery—results one commenter called “nearly miraculous” compared with long-term studies of efforts to prevent conversion through lifestyle change.
The retrospective study examined data from 1,326 bariatric patients with prediabetes who underwent Roux-en-Y gastric bypass or sleeve gastrectomy between 2001 and 2022. In total, 1,154 gastric bypass and 172 sleeve gastrectomy cases were included in the analysis. Nonsurgical patients from a primary care cohort propensity-matched on hemoglobin A1c, age, sex and body mass index were used as controls. Time to type 2 diabetes mellitus (T2DM) conversion in bariatric patients was estimated with the Kaplan-Meier analysis and compared in gastric bypass versus sleeve gastrectomy and bariatric surgery versus controls using Cox regression. The cohort was 83% female, with a mean age of 45.3 years and mean BMI of 46.9 kg/m2. Median follow-up was 7.2 years.
At five, 10 and 15 years postoperatively, the T2DM conversion rate was 1.8%, 3.3% and 6.7%, respectively, in the bariatric surgery group. Conversion rates in the nonsurgical group were much higher at five, 10 and 15 years: 31.1%, 51.4% and 68.7%, respectively (hazard ratio [HR], 19.8; 95% CI, 13.9-28.4; P<0.0001) (Figure 1). Stratifying by surgery type, sleeve gastrectomy patients were four times more likely to convert to T2DM compared with gastric bypass patients (HR, 4.01; 95% CI, 1.71-9.39; P=0.0014) (Figure 2).
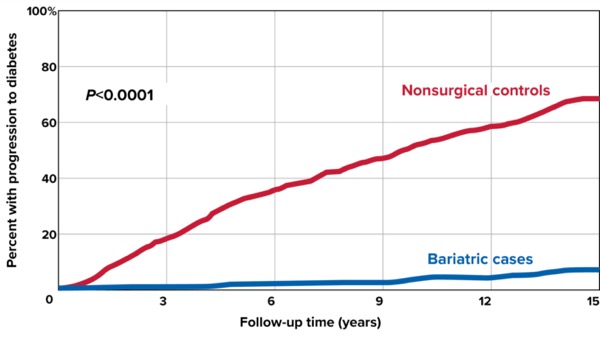
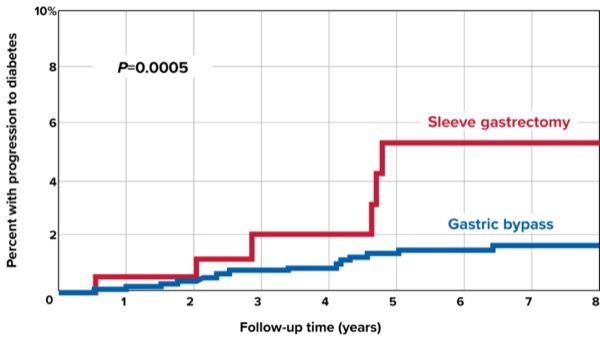
Figure 2. Progression to type 2 diabetes mellitis when comparing Roux-en-Y gastric bypass to sleeve gastrectomy.
Related Content


The study’s lead author, David M. Parker, MD, the bariatric surgery program director at Geisinger Medical Center, in Danville, Pa., said he expected to see lower conversion rates from prediabetes to T2DM in bariatric surgery patients compared with nonsurgical patients, but was surprised that the difference was so stark.
“Our primary hypothesis was that patients who underwent bariatric surgery would perform better in terms of not progressing to diabetes than those who did not have surgery,” Dr. Parker said. “We did not expect the difference to be so discrepant.”
The findings clearly underline the efficacy of bariatric surgery in preventing progression from prediabetes to T2DM, he said.
“Bariatric surgery has been the most successful medical treatment for T2DM for the past 25 years. Prediabetes is associated with class 3 obesity and diabetes,” Dr. Parker said. “The biggest takeaway from this study is that bariatric surgery is also the best medical strategy to prevent T2DM in patients with [prediabetes] and class 3 obesity.”
Matthew Brengman, MD, a bariatric surgeon at Advanced Surgical Partners of Virginia, in Richmond, acknowledged the limitations of the retrospective study but said the findings are striking.
“This study is not as powerful as a prospective study or a randomized controlled trial, but for this question it’s quite powerful,” Dr. Brengman said. “Given the known dramatic effect of bariatric surgery on diabetes, I suppose I’m not surprised by the results, but what’s remarkable is the magnitude of the effect.”
As a basis of comparison, Dr. Brengman cited the National Institute of Diabetes and Digestive and Kidney Diseases Diabetes Prevention Program Outcomes Study (DPPOS), a randomized controlled trial comparing lifestyle interventions versus twice-daily metformin versus standard dietary counseling initiated in 2002, with 15-year results available (www.repository.niddk.nih.gov/studies/dppos/).
“In DPPOS, 55% of individuals who underwent lifestyle intervention and 56% who continued to take metformin developed T2DM, compared with 62% of participants who took a placebo,” he said. “Through this lens, these results are not only remarkable but nearly miraculous.”
—Ajai Srinivas
Drs. Brengman and Parker reported no relevant financial disclosures.
Originally published by our sister publication General Surgery News