

WASHINGTON—Current guidelines suggest 60% to 76% of the U.S. population should be screened for metabolic dysfunction–associated steatotic liver disease, but refined criteria reducing the target screening population to about 22% would be safe and likely more practical, according to an analysis presented at The Liver Meeting 2025.
The investigators, led by Laurens van Kleef, MD, PhD, a postdoctoral researcher at Erasmus MC, in Rotterdam, Netherlands, looked at National Health and Nutrition Examination Survey data from 2017 to 2020 and identified 5,904 adults with a medical history indicating screening eligibility and a body mass index of at least 18.5 kg/m2 (abstract 2497). The investigators assessed the cohort for the presence of a liver stiffness measure (LSM) of at least 8 kPa and found that it was present in 8.9% of the population. They stratified this group of patients “across the full spectrum of current recommended screening indicators” and identified 80 potential subgroups, the Dr. van Kleef noted.
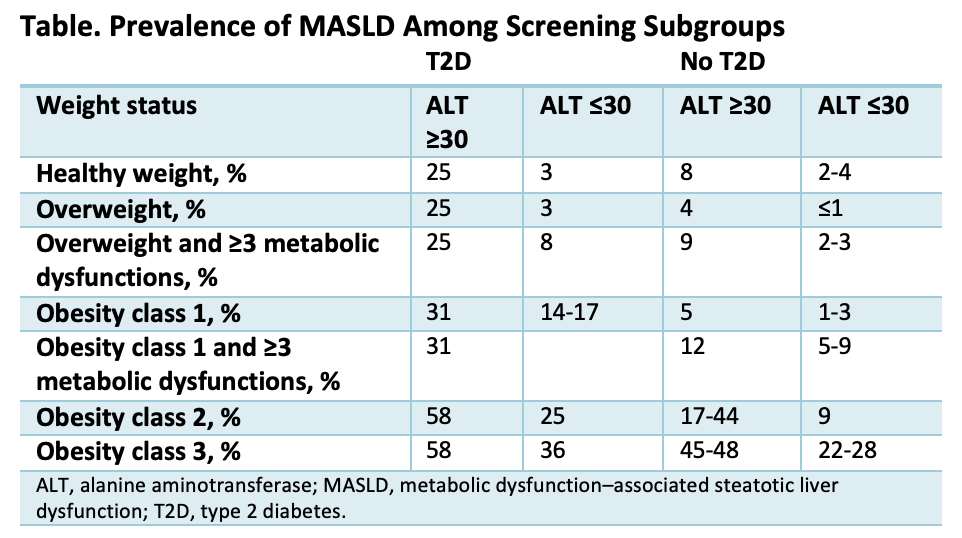
Among the 24% to 40% of the general population who do not meet the screening guidelines, the rate of LSM of at least 8 kPa is around 2%, which is similar to that in some subgroups in the analysis who are eligible for screening, Dr. van Kleef said (Table). For example, this would include adults with diabetes, normal alanine aminotransferase (ALT) levels (<30 IU/L), and no obesity, as well as those with obesity class 1 or 2, no diabetes, and normal ALT levels. Forgoing screening in these patient groups would allow for a more targeted, effective approach, according to the investigators.
The current guidelines-based screening strategy has a positive predictive value (PPV) of 11.1% to 13.5% for an LSM of at least 8 kPa. A refined screening strategy comprising 22% of the U.S. population would improve PPV to 27.7% for an LSM of at least 8 kPa and would have a negative predictive value of 96.3%, according to the analysis.
Dr. van Kleef acknowledged the irony of recommending screening fewer patients in a highly underdiagnosed disease but said underdiagnosis may be a clarion call to better stratify them and improve engagement of healthcare professionals in these targeted screening programs.
“As it is, these patients are barely getting screened,” he told Gastroenterology & Endoscopy News. “It’s important to be realistic and start with those at highest risk in our attempts to reach the patients who need diagnosis and treatment.”
—Katie Prince

