


CHICAGO—Maladaptive weight control and eating behaviors are associated with a significantly increased risk for irritable bowel syndrome in adulthood, according to new research.
While the research is new, the findings mimic what providers have seen in the real world, senior investigator Kyle Staller, MD, MPH, told Gastroenterology & Endoscopy News. “To our knowledge, these are the first data that show prospectively what we’ve always seen in the clinic: that a lot of our IBS patients have a history of disordered eating, though many have never had a diagnosis of an eating disorder,” said Dr. Staller, the director of the Gastrointestinal Motility Laboratory at Massachusetts General Hospital, in Boston.
Anthony Lembo, MD, the director of research for Cleveland Clinic’s Digestive Disease & Surgery Institute, who was not involved in the study, underscored the importance of the findings, saying they “absolutely” mirror what he’s seen in his own practice. “This is a one-of-a-kind study and a unique data set” that should get the attention of clinicians, said Dr. Lembo. “We have to recognize that disordered eating places patients at risk for IBS, and not only ask about diet but about eating behavior.”
Robust Associations
Although IBS is a common condition, prospective data of its early-life risk factors are limited. In this study, the investigators looked for precursors of IBS in the form of maladaptive weight control and eating behaviors in adolescence and young adulthood. They analyzed data collected for women in the GUTS (Growing Up Today Study) prospective cohort of girls aged 9 to 14 years (mean age, 12 years), which began enrolling in 1996. At baseline and during follow-up, participants reported how often they engaged in several maladaptive eating and weight control behaviors during the past year: never, ever, weekly or monthly.

From 1996 to 2013, self-reported behaviors were recorded, such as instances of self-induced vomiting, laxative use and fasting for the purpose of losing weight. From 2001 to 2013, the study also collected eating disorder diagnoses by providers, including binge eating, bulimia nervosa, anorexia nervosa and other eating disorders.
These “exposure data” were paired with incident IBS diagnoses as identified from four questionnaire cycles (2013, 2014, 2016, 2019). The final analysis included participants with complete data on IBS status and maladaptive eating and weight control behaviors. Disordered eating behaviors in the final sample included self-induced vomiting (n=5,740), laxative use (n=5,438), fasting (n=5,522), binge eating (n=4,459) and clinician-diagnosed eating disorders (n=5,316).
The investigators used multivariable logistic regression, adjusting for age, body mass index and depressive symptoms, to estimate odds ratios and 95% CIs for IBS risk.
The researchers, led by Keming Yang, MD, PhD, identified 4,913 participants without a diagnosis of an eating disorder, of whom 90 developed IBS. A total of 403 had a diagnosis of an eating disorder, of whom 37 developed IBS. Thus, the odds of developing IBS among those with maladaptive eating were over three times as high as in those without maladaptive eating (OR, 3.42; 95% CI, 2.38-4.90), Dr. Staller reported at Digestive Disease Week 2023 (abstract Tu1622).
Compared with adolescents and young adults who never engaged in these behaviors, each maladaptive weight control and eating behavior was associated with an increased risk for future IBS, with increased performance of each of these behaviors associated with a greater magnitude of IBS risk (Table).
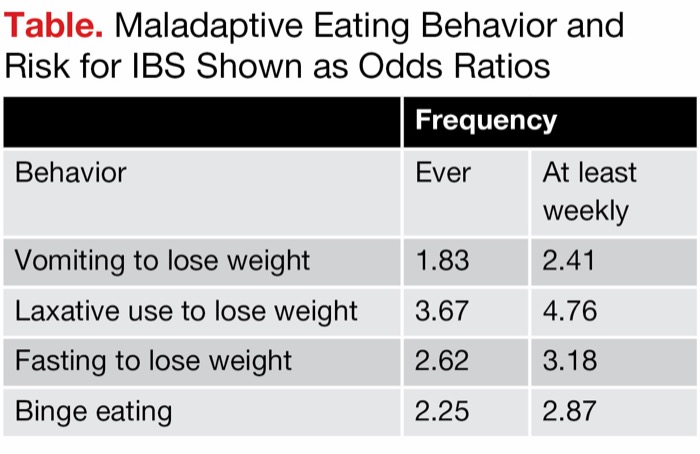
| Table. Maladaptive Eating Behavior and Risk for IBS Shown as Odds Ratios | ||
| Frequency | ||
|---|---|---|
| Behavior | Ever | At least weekly |
| Vomiting to lose weight | 1.83 | 2.41 |
| Laxative use to lose weight | 3.67 | 4.76 |
| Fasting to lose weight | 2.62 | 3.18 |
| Binge eating | 2.25 | 2.87 |
Why This Matters
Although current guidance does not recommend screening of eating disorders—specifically the U.S. Preventive Services Task Force’s guidelines—Dr. Staller maintained that the findings of his study suggest screening should be done. He said providers should note the crossover between dietary interventions for IBS, which can be restrictive, and disordered eating. He said he often sees young women who have been put on restrictive diets to control IBS symptoms, but this may not be advisable for those recovering from an eating disorder. “Even if the patient is in recovery, prescribing a restrictive diet can retrigger some of the abnormal cognitions of the eating disorder or the patient can develop a different eating disorder, avoidant restrictive food intake disorder, or ARFID,” Dr. Staller said. “The worst thing you can do is to start a restrictive diet in a person with a history of disordered eating.”
For these patients, Dr. Staller suggested that the menu of IBS treatment options should exclude restrictive diets. While a patient may have some “trigger” foods, this must be accompanied by sensitivity to those triggers, he said. “We need to target the sensitivity, such as with neuromodulators, gut-directed behavioral therapy and drugs approved for treating IBS. It’s great to have dietary options, such as low-FODMAP [fermentable oligosaccharides, disaccharides, monosaccharides and polyols] diets, but we have to use these responsibly.”
—Caroline Helwick
Dr. Lembo reported financial relationships with Aeon, BioAmerica, Eurogastrx, Evoke Pharma, Focus Med, Gemelli, Ironwood, OrphoMed, Pfizer, Salix, Takeda and Vibrant. Dr. Staller reported financial relationships with Anji, Ardelyx, GI Supply, Restalsis and Sanofi.



This article is from the September 2023 print issue.