

Although proton pump inhibitors are a mainstay in preventing cancer in patients with Barrett’s esophagus, 56% of these patients fall off PPI adherence during the year following BE diagnosis, a new analysis has revealed.
The study also found predictors of poor adherence, including new use of PPIs, male sex and specific comorbidities.
“Our findings have implications for BE care management,” noted the researchers, who were led by Charles Gaber, MPH, PhD, an assistant professor in the Department of Pharmacy Systems, Outcomes and Policy at the University of Illinois at Chicago (Pharmacoepidemiol Drug Saf 2024;33[2]:e5760). Specifically, “adherence to prescription PPIs is heterogeneous within the BE population” and interventions to improve adherence should be tailored, they indicated.
Dr. Gaber and his co-investigators retrospectively examined a large commercial and healthcare utilization database, identifying 79,701 adults diagnosed with BE between 2010 and 2019. Patients had filled a PPI prescription within 60 days of BE diagnosis and had insurance coverage during the entire year before and the year after BE diagnosis.
The study population was divided according to history of PPI use, with 54.3% using PPIs at the time of BE diagnosis, 16.9% having a history of PPI use but not at the time of BE diagnosis and 28.7% receiving PPIs for the first time after BE diagnosis.
A range of covariates were included in the analysis, such as demographic characteristics, the year of diagnosis, geographic region, insurance type, prior healthcare utilization, comorbidities and use of other chronic medications.
The patients were a median 53 years of age at the time of diagnosis and 57% were male. In the year prior to BE diagnosis, 28% had received one to two additional chronic medications, 22% had filled prescriptions for three to four chronic medications and 36% had filled prescriptions for five or more chronic medications. The remainder had not filled prescriptions for additional chronic medications.
The investigators found five medication patterns in the population in the year after BE diagnosis: consistently high adherence (44% of the population), a moderate decline in adherence (18%), a slow decline (12%), a rapid decline (10%) and a decline followed by a return to adherence (16%).
Several variables predicted adherence. For example, those already using PPIs at the time of BE diagnosis were 58% less likely than new PPI users to have a moderate decline in adherence (odds ratio [OR], 0.42; 95% CI, 0.40-0.44). However, those with a history of PPI use (but who were not taking PPIs at the time of diagnosis) were more likely than new users to have a decline in PPI adherence (moderate decline vs. consistently high group: OR, 1.30; 95% CI, 1.22-1.39).
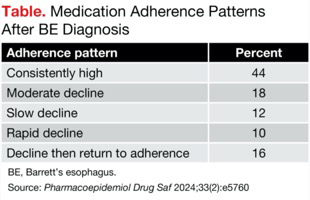
| Table. Medication Adherence Patterns After BE Diagnosis | |
| Adherence pattern | Percent |
|---|---|
| Consistently high | 44 |
| Moderate decline | 18 |
| Slow decline | 12 |
| Rapid decline | 10 |
| Decline then return to adherence | 16 |
| BE, Barrett’s esophagus. | |
Male sex also was associated with adherence, with males 34% less likely to have moderate declines in adherence than females (OR, 0.66; 95% CI, 0.63-0.69). The researchers also linked past use of preventive medical services and the use of at least one chronic medication at the time of diagnosis to a higher likelihood of complete adherence (one preventive visit: OR of moderate decline, 0.81; 95% CI, 0.77-0.85; one to two chronic drugs: OR of moderate decline, 0.59; 95% CI, 0.55-0.63).
An anxiety diagnosis also predicted a decline in adherence (moderate decline: OR, 1.17; 95% CI, 1.07-1.28; slow decline: OR, 1.15; 95% CI, 1.04-1.28; rapid decline: OR, 1.26; 95% CI, 1.12-1.41). Similarly, those with diabetes were more likely to experience a decline in adherence in the year after BE diagnosis (moderate decline: OR, 1.10; 95% CI, 1.02-1.19; slow decline: OR, 1.09; 95% CI, 1.00-1.18; rapid decline: OR, 1.38; 95% CI, 1.25-1.52).
Tailored Interventions May Be Needed
“Individuals predicted to be in the fast decline group may need different interventions to promote adherence than those who disengage from therapy after a period of adherence,” according to Dr. Gaber and his co-investigators. “For instance, an intervention based on the health belief model to increase perceived severity of esophageal cancer and perceived benefits of PPIs may be more effective [in this group], whereas reminder calls may be more effective for individuals disengaging from PPIs more slowly.”
Although the researchers did not explore why some patients experienced a decline and then returned to adherence, they speculated it may have been due to “scheduled check-in visits with prescribers or longitudinal changes in symptom burden.”
One possibility the study could not account for was that some patients switched to over-the-counter PPIs. However, “our supplemental analysis suggested OTC PPIs are usually not cheaper” than prescription PPIs, the researchers wrote, so there wouldn’t be an easy financial benefit for switching to OTC drugs.
Asked to comment, Prateek Sharma, MD, a professor of medicine at the University of Kansas, in Kansas City, told Gastroenterology & Endoscopy News that he has seen patients struggle with adherence firsthand. “I do agree that compliance with PPIs is an issue not just for BE patients but for [gastroesophageal reflux disease] patients in general,” he said. In his personal experience, BE patients have better adherence than GERD patients without BE, he said. “However, these results do not surprise me.”
It’s important to have patients with BE continue PPIs, he continued, to reduce the risk for esophagitis, ulceration, and even dysplasia and strictures.
This new information about risk factors can help physicians home in on who may need a little extra help, Dr. Sharma said. “As physicians, we can emphasize more to these patients [the need] to continue.”
—David Wild and Meaghan Lee Callaghan
Drs. Gaber and Sharma reported no relevant financial disclosures. Dr. Sharma is a member of the Gastroenterology & Endoscopy News editorial board.



This article is from the April 2024 print issue.