

SAN DIEGO—Getting to the root of reflux and successfully treating it is a perennial challenge for gastroenterologists. C. Prakash Gyawali, MD, a professor of medicine and the director of the neurogastroenterology and motility program at Washington University in St. Louis, offered some guidance on managing gastroesophageal reflux disease in a presentation at DDW 2025.
Document It!
“The more atypical the symptom, the more you need to document that reflux is actually occurring. There are often confounders for symptoms that are important to look for,” Dr. Gyawali said.
The means of testing should be based on the patient’s presentation. For a patient with typical symptoms of heartburn, regurgitation, or esophageal chest pain, an empirical trial of antisecretory therapy is reasonable, but Dr. Gyawali said he does not hesitate to advance to a physiologic evaluation. The preferred test is wireless pH monitoring, but pH-impedance monitoring with high-resolution manometry (HRM) also is a reasonable option.
For patients with the atypical symptoms of belching, chronic cough, or asthma, the likelihood of GERD is lower than with typical symptoms. Dr. Gyawali said he performs endoscopy followed by pH-impedance monitoring and HRM to identify or rule out reflux. The atypical symptoms of hoarseness, globus, nausea, abdominal pain, and dyspepsia also are much less likely to indicate GERD, he said, and up-front testing typically is performed to rule out GERD when needed, with laryngoscopy possibly considered first for throat symptoms.
“It is well worth evaluating atypical symptoms up front rather than after a trial of a proton pump inhibitor. … And it’s well worth knowing when endoscopy is going to be useful,” Dr. Gyawali said. “So, in patients with esophageal symptoms, especially with atypical symptoms or incomplete response to PPIs and many other situations, endoscopy off PPIs can help make the case for reflux disease if certain findings are encountered.” Some of these findings include peptic stricture, Barrett’s esophagus, and advanced grade esophagitis. When symptoms other than reflux are identified, these disorders should be treated, he added.
For a finding of normal mucosa or Los Angeles grade A, a 96-hour wireless study may be diagnostic. LA grade B has a broad spectrum, and when a finding is “borderline,” it is reasonable to evaluate reflux burden. Emerging data suggest short studies (48 hours) may be sufficient, he said.
“The intent is to determine if GERD exists,” he said. In the absence of proven GERD, there typically is a “broad inconclusive swatch” for which metrics from adjunctive tests can be informative.
Confounders of Response To Medical Management
When patients are on a PPI regimen, there are several reasons for a suboptimal response, a common one being inadequate or improper dosing. When this is suspected, Dr. Gyawali recommended dosing PPIs 30 to 60 minutes before meals, dosing twice daily, switching to a more potent PPI, considering a potassium-competitive acid blocker (PCAB), and, for patients taking suboptimal doses out of concern for side effects, addressing safety concerns.
Patients with regurgitation-predominant GERD frequently respond poorly to PPIs, and may have large hiatal hernias or a disrupted esophagogastric junction (EGJ) barrier. For these patients, invasive GERD management using mechanical therapies is more effective than PPIs. He recommended fundoplication and possibly transoral incisionless fundoplication, magnetic sphincter augmentation, or Roux-en-Y gastric bypass, depending on the clinical scenario.
Superimposed functional disorders (e.g., esophageal hypersensitivity and hypervigilance), behavioral conditions (supragastric belching and rumination syndrome), and affective disorders (depression, anxiety) also can confound PPI response. Patients with these conditions are not likely to see improvement with treatment but may respond to adjunctive approaches.
Dr. Gyawali’s recommendations were to optimize medical management of GERD, reinforce lifestyle and behavioral options, consider neuromodulators for overlapping disorders of the gut–brain axis, and consider cognitive behavioral therapy and diaphragmatic breathing exercises.
Algorithm for Standard Management
Dr. Gyawali stressed the importance of first confirming the diagnosis of GERD. He reminded DDW attendees, “The more atypical the symptom, the greater the need for documentation of an abnormal reflux burden prior to long-term GERD management.”
If the “simple PPIs” are ineffective, he recommended “moving up the potency ladder,” and listed these omeprazole equivalents (1.00) for the available agents: pantoprazole, 0.23; lansoprazole, 0.90; esomeprazole, 1.60; rabeprazole, 1.82. Along with optimal PPI dosing (or switching to PCABs), medical optimization can include lifestyle and diet adjustments, postural management, adjunctive alginates or baclofen, and treatment of hypervigilance and affective disorders.
For GERD patients with severe reflux esophagitis (LA grade C or D) who have not healed on optimized double doses of PPIs, PCABs can be good options. This is especially true for patients who are not good candidates for anti-reflux procedures due to comorbidities, those with motility issues (esophageal and gastric), and those with persistent symptomatic reflux, he said.
A number of clinical trials have demonstrated noninferiority of PCABs to PPIs in esophagitis healing overall and in maintenance of healing and superiority to PPIs in advanced-grade esophagitis, he said (Gastroenterology 2023;164[1]:61-71; Aliment Pharmacol Ther 2019;49[7]:864-872; Aliment Pharmacol Ther 2023;57[1]:72-80). In addition, PCABs outperformed placebo in heartburn relief in the absence of esophagitis (Clin Gastroenterol Hepatol 2024;22[11]:2211-2220.e10).
Escalation to Anti-Reflux Surgery
In well-characterized GERD, surgical and medical therapy can be equivalent, making surgery an option in certain patients. This choice should be informed by body habitus, comorbidities, and available surgical expertise.
In some patient subsets, anti-reflux surgery is “potentially” necessary, a category supported by a study that found surgery was significantly more effective (67%) than medical management (28%) in patients with proven GERD that was medically refractory (P=0.007) (N Engl J Med 2019;381[16]:1513-1523). “We say ‘potentially necessary’ because PCABs might change this perspective a bit,” Dr. Gyawali commented. In evaluating patients for the “potentially necessary” category, one must assess for achalasia spectrum disorders, esophageal peristaltic performance, and EGJ disruption, he added.
For patients with a disrupted EGJ barrier, especially those with a large hiatal hernia, surgery can be considered “necessary,” as it brings patients considerable symptomatic relief (Br J Surg 2013;99:1315-1321). “Especially in patients who have postprandial symptoms, shortness of breath, anemia, and early satiety, anti-reflux surgery may be a necessity,” he said.
Esophageal motor function also should be assessed. Normal manometry is the most common pattern in GERD, but it is important to exclude achalasia in PPI nonresponders, which can be present despite normal integrated relaxation pressure. A heterogeneous condition called EGJ outflow obstruction also could be occurring, and adjunctive testing before anti-reflux surgery can help define this.
Use of HRM Before Surgery
An international initiative of surgeons and gastroenterologists published a consensus statement, The Padova Classification, to refine the use of HRM before and after anti-reflux surgery (Ann Surg 2025;281[1]:124-135). Dr. Gyawali, who was a co-author, summarized its key points and recommendations:
- HRM is essential for ruling out achalasia before surgery.
- The etiology of EGJ outlet obstruction needs to be defined before surgery.
- HRM can provide baseline EGJ metrics useful in planning surgery.
- Hypercontractility without obstruction can be seen with GERD.
- Distal esophageal spasm with dysphagia/chest pain could be achalasia type 3.
- Distal esophageal spasm with reflux symptoms can be compatible with GERD.
- HRM can provide baseline EJG metrics useful in planning surgery.
Selecting Patients for Surgery
The ICARUS guidelines (Gut 2019;68[11]: 1928-1941) list favorable and unfavorable phenotypes of patients for anti-reflux surgery. Favorable factors include typical symptoms and good PPI response; symptoms in the presence of hiatal hernia, Barrett’s esophagus, and LA grade B esophagitis or higher; and symptoms in the presence of axial hiatal hernia and/or paraesophageal hernia on imaging.
In other words, the favorable phenotype has “good evidence of reflux,” Dr. Gyawali said. The favorable subset does not exclude patients with morbid obesity, substance abuse, or short esophagus, “but patients should be off whatever substance they abuse,” he added.
Unfavorable phenotypes include patients with functional heartburn and eosinophilic esophagitis and those with normal pH monitoring off PPI therapy.
Endoscopy within the past year is strongly recommended. Manometry and esophageal pH or pH-impedance monitoring are mandatory before anti-reflux surgery (off therapy in nonerosive reflux disease, but patients can be on therapy with prior GERD evidence). Routine biopsies of the distal esophagus and a routine gastric emptying assessment are not needed. Barium radiography should be obtained when hiatal hernia or short esophagus are suspected, he said.
Know the Spectrum
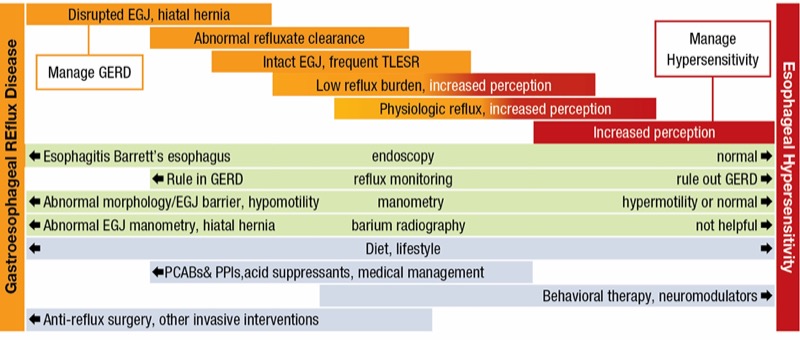
“In the end, it’s important when we evaluate the patient to know where in the spectrum the patient lies,” Dr. Gyawali said (Figure).
From a pathophysiologic standpoint, the clearest reflux patients will be on one end of the spectrum. These are the patients who have abnormal findings on endoscopy and reflux monitoring, and in whom escalation to anti-reflux surgery will be most likely. In these patients, the aim is to manage acid exposure. On the other end of the spectrum are those patients in whom the aim is to manage hypersensitivity. In these patients, there is a greater need for interventions such as behavioral therapy and neuromodulators.
“For all patients, to varying degrees, other options in management can include diet and lifestyle modifications,” he added. “And remember that hypervigilance can permeate the entire spectrum of anti-reflux management.”
—Caroline Helwick
Dr. Gyawali reported financial relationships with Alimentiv, Braintree, Carnot, Diversatek, and Medtronic.



This article is from the November 2025 print issue.