

Division of Gastroenterology and Hepatology
Medical Director, Digestive Health Center
MetroHealth
Cleveland, Ohio
In this two-part column, I highlight seven studies presented at DDW 2025. In this part, I discuss studies on a new functional lumen imaging probe (FLIP) panometry–based motility classification algorithm and new potassium-competitive acid blocker (PCAB). In part 1 last month, I reviewed studies on anti-reflux procedures and the cost-effectiveness of proton pump inhibitor therapy. The first study I highlight this month is a pivotal trial conducted in India comparing the PCAB fexuprazan with esomeprazole for the healing and symptom control of erosive esophagitis. The study demonstrated that fexuprazan was noninferior to esomeprazole in this patient population. I also highlight two additional abstracts on an updated version (2.0) of the FLIP Panometry Motility Classification that aims to establish a standardized approach, vocabulary and interpretation for the procedure.
Fexuprazan Versus Esomeprazole For Erosive Esophagitis
DDW 2025 New and Novel Approaches to GERD Management Session, abstract 1150
Investigators compared the PCAB fexuprazan (Daewoong) with the PPI esomeprazole in patients with erosive esophagitis (EE) in a phase 3, randomized controlled trial across 20 sites in India (Clinical Trials Registry – India ID: CTRI/2024/02/062543).
Eligible patients were 18 to 65 years of age, had EE and were Los Angeles classification grades A to D, and had heartburn or regurgitation symptoms on at least one day in the previous week. In total, 210 patients, stratified by LA classification, were randomized 1:1 to receive daily doses of either 40 mg of fexuprazan plus placebo (for esomeprazole) or 40 mg of esomeprazole plus placebo (for fexuprazan). Patients were assessed at baseline as well as weeks 4, 8 and 10. Efficacy was assessed in the 200 patients who completed the study per protocol (n=101 fexuprazan; n=99 esomeprazole). Safety was assessed in the full population. The primary end point was the proportion of patients with endoscopically confirmed healed EE by eight weeks. If patients achieved endoscopic healing by week 4, treatment was stopped, and the patients were followed for an additional two weeks to assess safety.
Patients in each arm were comparable across key demographic and disease characteristics, including gender (~70% male), age (~41 years), body mass index (~25 kg/m2), LA grade (~53% A, ~34% B, ~12% C, ~1% D), Frequency Scale for the Symptoms of GERD (FSSG) score (~24) and GERD Health-Related Quality of Life (GERD-HRQOL) score (~23).
At week 8, 95.05% of fexuprazan and 92.93% of esomeprazole patients met the primary end point (difference, 2.12%; 95% CI, –4.47% to 8.71%), indicating noninferiority of fexuprazan. Similarly, at week 4, the proportion of patients who achieved healing was comparable (48.51% vs. 50.51%; difference, –1.99%; 95% CI, –13.64% to 11.37%).
The proportions of patients in each arm who had 24-hour, daytime or nighttime heartburn-free days were comparable across arms at each time point: baseline, week 4 and week 8. This same pattern held for regurgitation-free days. Changes in FSSG and GERD-HRQOL scores from baseline to week 4 and baseline to week 8 also were similar across treatment arms.
Adverse events were seen in 20% of fexuprazan and 21% of esomeprazole patients. Three patients in the fexuprazan arm and four in the esomeprazole arm had drug-related treatment-emergent adverse events (TEAEs), including diarrhea, dizziness, headache and vomiting. Two patients in each arm had TEAEs that led to dose interruptions, but there were no serious TEAEs and none that led to discontinuation.
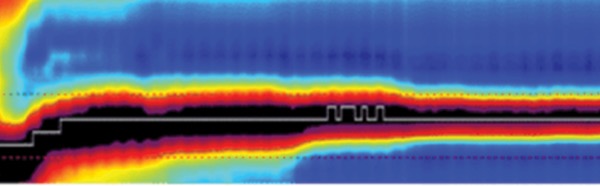
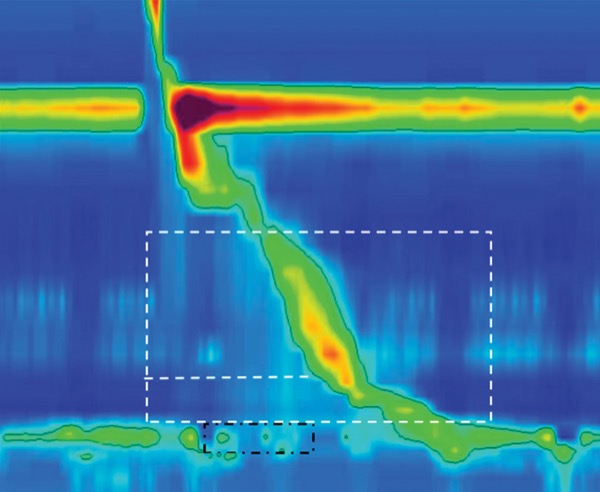
FLIP Panometry Classification for Esophageal Motility Assessment Version 2.0
DDW 2025 Advances in Esophageal and Foregut Endoscopy Session, abstract 103
A team of 19 FLIP panometry experts convened to develop a version 2.0 of the FLIP Panometry Motility Classification and formalize a “standardized approach, vocabulary and interpretation of the procedure.”
Initially, three members drafted statements, which the rest of the working group voted on using a scale of 1 to 9. Scores of 7 or higher indicated the statement was “appropriate,” and consensus was defined as at least 80% of votes greater than/equal to 7. Between rounds of voting, statements were discussed and revised.
Ultimately, the working group reached consensus on 40 statements and the motility classification scheme (Gastroenterology 2025;168[6]:1114-1127): Fifteen statements related to FLIP panometry protocol, three pertained to esophagogastric junction (EGJ) opening interpretation (normal, inconclusive or reduced), and 15 were in regard to contractile response interpretation (normal, spastic, disordered, diminished or absent).
Key statements include:
- “FLIP panometry should be interpreted in the context of the clinical presentation, the accompanying esophagogastroduodenoscopy findings and other relevant complementary testing.”
- “A major motor disorder is unlikely in the setting of a ‘normal’ FLIP panometry classification (i.e., normal contractile response with [normal EGJ opening]).”
- “Diminished or absent contractile response with reduced esophageal opening supports the diagnosis of a disorder of EGJ outflow.”
- “A spastic or inconclusive FLIP panometry classification should prompt further workup such as with high-resolution manometry [HRM] and/or timed barium esophagram with tablet.”
Validation of FLIP Panometry Classification For Esophageal Motility Version 2.0
DDW 2025 Oropharyngeal and Esophageal Motility Disorders Session, abstract 1042
Researchers at Northwestern University and Baylor University validated the updated FLIP 2.0, comparing motility diagnoses relative to HRM and Chicago Classification version 4.0 (CCv4.0) and comparing FLIP 2.0 classifications with FLIP 1.0 classifications.
The investigators included patients evaluated at two participating health systems who underwent FLIP and HRM between 2020 and 2024 without any previous or intervening endoscopic or surgical intervention. Patients were ineligible if they had mechanical obstruction or previous foregut surgery/endoscopic intervention.
Patients with inconclusive HRM diagnoses underwent timed barium esophagram (TBE) to classify findings based on CCv4.0. Abnormal TBE indicated conclusive EGJ outlet obstruction (EGJOO), normal TBE indicated normal esophageal motility and inconclusive TBE indicated an inconclusive diagnosis. Those with inconclusive TBE were excluded from primary analyses.
In total, 805 patients were included in the study. The mean age of participants was 55 years and 62% were female. The primary indication for testing was dysphagia (74%). Inconclusive HRM diagnosis was found in 101 patients.
When comparing the FLIP 2.0 classifications with HRM and CCv4.0 motility diagnoses, the investigators found that, among the patients with normal FLIP 2.0 classification (n=137), 93% had normal motility or ineffective esophageal motility on HRM, none had achalasia on HRM, and two had EGJOO on HRM. Normal FLIP 2.0 indicated a negative predictive value of 99% for disorders of EGJ outflow.
In addition, among patients with non-spastic obstruction FLIP 2.0 classification (n=163), 91% had a conclusive disorder of EGJ outflow on HRM.
Related Content



Finally, among patients with spastic obstruction FLIP 2.0 classification (n=76), 16 had type III achalasia on HRM, which represented 43% of patients with type III achalasia on HRM.
The investigators also compared FLIP 2.0 versus 1.0 classifications. Patients classified in FLIP 1.0 as having obstruction with weak contractile response were now split to being classified as spastic obstruction or non-spastic obstruction in FLIP 2.0, with the former including more of the type III achalasia patients and the latter more of the type I and II achalasia patients. Patients classified in FLIP 1.0 as having weak motility were now split to being classified as hypocontractile or possible spasm in FLIP 2.0, with the former including more patients with absent contractility on HRM and the latter more patients with hypercontractility on HRM. Ineffective esophageal motility on HRM was relatively evenly split across the hypocontractility and possible spasm FLIP 2.0 classifications. Finally, patients classified in FLIP 1.0 as being spastic reactive were now split into being classified as spastic obstruction, possible obstruction or possible spasm in FLIP 2.0, with spastic obstruction including the greatest proportion of patients with type III achalasia on HRM who were classified as spastic reactive in FLIP 1.0.
The investigators noted the strength of FLIP 2.0 over 1.0 for “differentiating non-spastic from spastic achalasia and possibly identifying relevant hypocontractility.” In addition, they noted that these results indicate that FLIP 2.0 “accurately categorized esophageal motility, aligning with CCv4.0.” Taken together, according to the investigators, “FLIP 2.0 validly complements or may serve as an alternative to HRM for diagnosis of esophageal motility disorders.”
This article is from the August 2025 print issue.