

WASHINGTON—Despite recommendations to adequately photo-document large polyps, a study from Cleveland Clinic found that only about half of such polyps are so documented before and after resection, virtually none include a measuring tool adjacent to the polyp in the photo, and up to 25% described by the proceduralist as at least 10 mm in size actually may be smaller.
The U.S. Multi-Society Task Force (USMSTF) strongly recommends photo documentation of all lesions at least 10 mm in size before removal and suggests that providers capture an image showing polyp size relative to an open forceps or open snare of known size (Am J Gastroenterol 2020;115[3]: 415-434). In their guideline, USMSTF also strongly suggests that providers photo-document the polyp resection defect after resection.
In 2023, Khan et al conducted a study on 1,693 polyps at least 10 mm in size removed in 1,322 colonoscopies by 25 endoscopists in the Cleveland Clinic Health System from 2016 to 2021 (Gastrointest Endosc 2023;98[5]:797-802). A review of all procedures showed that photo documentation occurred in 82% before resection, 52% after resection, and 48% both pre- and post-resection. Neither the Khan study nor the USMSTF discussed the quality of the photo documentation.
In the new study, presented at DDW 2024, investigators aimed to assess the quality of pre- and post-resection photo documentation of polyps at least 10 mm in size, randomly selected from the 1,693 in the previous Cleveland Clinic study (abstract 208).
Related Content



After a training session, four independent endoscopists with a range of experience determined the quality of the photos and how often polyp size was verified relative to an open forceps or open snare and also analyzed the agreement on estimated size (=10 vs. <10 mm). The investigators, led by Anthony Kerbage, MD, an internal medicine resident at Cleveland Clinic, in Cleveland, along with Carol A. Burke, MD, a gastroenterologist at Cleveland Clinic and a past president of the American College of Gastroenterology, evaluated both pre- and post-resection documentation. They noted that before resection high-quality documentation provides information that guides accurate surveillance colonoscopy intervals, and post-resection, it confirms the complete removal of large polyps, which diminishes the risk for recurrence and protects against interval colorectal cancers.
The reviewers were a third-year GI fellow (reviewer 1), a gastroenterologist with two years of practice (reviewer 2), a gastroenterologist with eight years of practice (reviewer 3) and a gastroenterologist with 33 years of practice (reviewer 4).
The investigators found that the ratings of the quality of pre-resection and post-resection photo documentation varied across the four endoscopist reviewers (Table).
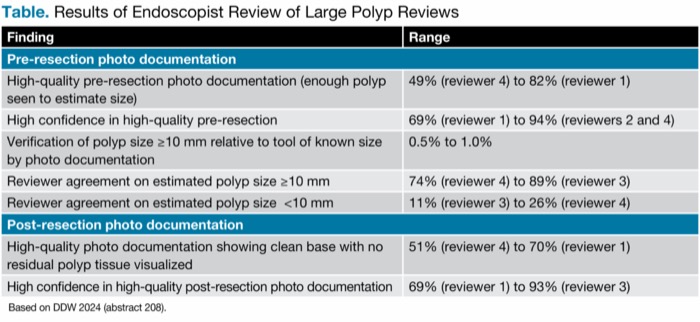
| Table. Results of Endoscopist Review of Large Polyp Reviews | |
| Finding | Range |
|---|---|
| Pre-resection photo documentation | |
| High-quality pre-resection photo documentation (enough polyp seen to estimate size) | 49% (reviewer 4) to 82% (reviewer 1) |
| High confidence in high-quality pre-resection | 69% (reviewer 1) to 94% (reviewers 2 and 4) |
| Verification of polyp size =10 mm relative to tool of known size by photo documentation | 0.5% to 1.0% |
| Reviewer agreement on estimated polyp size =10 mm | 74% (reviewer 4) to 89% (reviewer 3) |
| Reviewer agreement on estimated polyp size <10 mm | 11% (reviewer 3) to 26% (reviewer 4) |
| Post-resection photo documentation | |
| High-quality photo documentation showing clean base with no residual polyp tissue visualized | 51% (reviewer 4) to 70% (reviewer 1) |
| High confidence in high-quality post-resection photo documentation | 69% (reviewer 1) to 93% (reviewer 3) |
| Based on DDW 2024 (abstract 208). | |
The researchers said they want to further study the effects of high-quality photo documentation and evaluate better definitions of quality metrics for photo documentation. In addition, Dr. Kerbage said they want to evaluate the use of objective measuring tools, noting that “visual size estimation alone is imprecise and variable.”
Taking the Next Step
Brian Hanson, MD, the chief of the Gastroenterology Section at the Minneapolis VA Health Care System, said the findings are interesting but need to be logically applied. “It makes sense to take these pictures, but who actually sees them? Say, for example, this polyp is really more than 10 mm, then the patient should have every–two-year follow-up. There are probably a lot of patients being followed every three years, not based on polyp size but on the practitioner’s risk tolerance, or more cynically financial incentives, when we have scarce resources.”
He asked Dr. Kerbage how photo documentation, if serving as a quality metric, could be “operationalized” so that it informs the surveillance recommendations for individual patients. In response Dr. Kerbage said, “We assume that high-quality photo documentation improves outcomes, but there are no data on this. This is something to be done in the future. For now, it’s not enough to just document. We need to document with better quality.”
—Caroline Helwick
Drs. Hanson and Kerbage reported no relevant financial disclosures.
This article is from the September 2024 print issue.