


University of Kansas
School of Medicine
Kansas City
This month, Sharma’s Endoscopy Insights addresses quality in colonoscopy, particularly related to two important factors: serrated polyps and bowel preparation. I discuss two studies highlighting these factors.
There has been much interest in serrated polyps because they are an important precursor to colorectal cancer (CRC), but also because they can be flat, right-sided and easily missed during colonoscopy. This large, multicenter study revealed that patients who are white, smoke and have obesity are at increased risk for precancerous serrated polyps.
Adequate bowel preparation is a critical quality indicator for both colonoscopy and endoscopic examination. Unfortunately, some patients continue to have poor bowel prep before colonoscopy, negating the benefits of the procedure. This comprehensive meta-analysis revealed socioeconomic factors, patient factors and medication-related factors associated with inadequate bowel prep. These findings could help identify patients at high risk for inadequate bowel preparation before colonoscopy.
Serrated Polyps
Am J Gastroenterol 2024;119:2532–2539
In this multicenter, colonoscopy-based study, researchers investigated risk factors for serrated polyps in 6,278 participants in the Great Lakes/New England Clinical Validation Center Study, a multicenter CRC biomarker validation study. There were 565 patients with at least one serrated polyp, including 562 with sessile serrated lesions (SSL) and three with traditional serrated adenomas. Approximately 75% of participants enrolled between 2011 and 2017, and the remainder enrolled between 2018 and 2019.
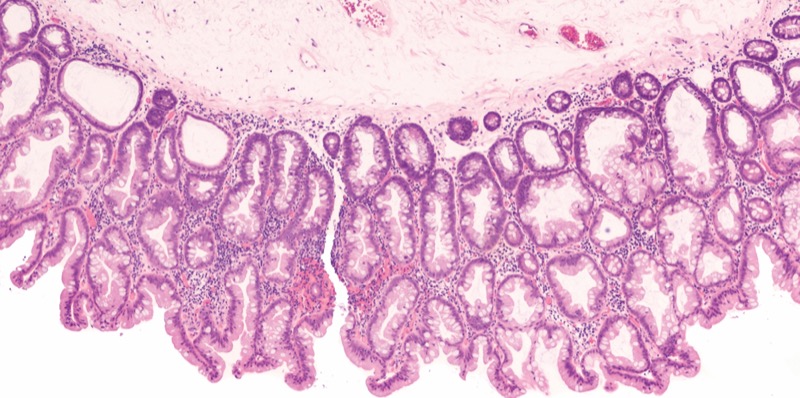
In the analysis, the investigators found that three factors were associated with SSL: white race (vs. Black race: adjusted odds ratio [aOR], 4.64; 95% CI, 1.89-11.41), obesity (body mass index [BMI] =30 vs. <25 kg/m2; aOR, 1.84; 95% CI, 1.42-2.39), and smoking (current vs. never smokers: aOR, 2.89; 95% CI, 1.97-4.23).
The authors concluded that their findings offer insight into which patients should be targeted for risk mitigation.
Bowel Preparation
Am J Gastroenterol 2024;119:2389-2397
In this systematic review and meta-analysis, U.S. researchers investigated sociodemographic and comorbidity-, medication-, preparation- and procedure-related risk factors for suboptimal prep.
The researchers identified 154 studies from the PubMed, Embase and Web of Science databases that included 358,257 patients and analyzed 48 risk factors that were assessed in three or more studies. In total, 54 of the studies were retrospective, 99 were prospective, and one had both prospective and retrospective cohorts. Across the studies, the rate of inadequate bowel preparation was 14.3% (149 studies).
Sociodemographic risk factors for inadequate prep were Medicaid insurance (OR, 2.07; 95% CI, 1.51-2.83), current tobacco use (OR, 1.33; 95% CI, 1.23-1.44), Black race (OR, 1.29; 95% CI, 1.11-152), low education level (OR, 1.26; 95% CI, 1.08-1.46), male sex (OR, 1.23; 95% CI, 1.17-1.29), unmarried status (OR, 1.22; 95% CI, 1.10-1.35), age 65 years or older (OR, 1.30; 95% CI, 1.07-1.57) and BMI 30 kg/m2 or higher (OR, 1.42; 95% CI, 1.19-1.70).
Comorbidity-related risk factors for inadequate prep were any psychiatric disease (OR, 2.46; 95% CI, 1.47-4.14), liver cirrhosis (OR, 2.43; 95% CI, 1.58-3.73), American Society of Anesthesiologists physical status III or greater (OR, 2.25; 95% CI, 1.37-3.69), poor functional status (OR, 2.13; 95% CI, 1.55-2.94), constipation (OR, 1.95; 95% CI, 1.71-2.21), diabetes mellitus (OR, 1.79; 95% CI, 1.62-1.98), previous abdominopelvic surgery (OR, 1.71; 95% CI, 1.33-2.20) and hematochezia (OR, 1.57; 95% CI, 1.33-2.20).
Medication-related risk factors for inadequate prep included tricyclic antidepressant use (OR, 2.41; 95% CI, 1.48-3.92), antidepressant use (OR, 1.69; 95% CI, 1.10-2.61), opioid use (OR, 1.56; 95% CI, 1.37-1.78), and calcium channel blocker use (OR, 1.39; 95% CI, 1.10-1.76).
Prep- or procedure-related risk factors were brown liquid rectal effluent (OR, 4.71; 95% CI, 2.82-7.90), any incomplete bowel prep intake (OR, 3.27; 95% CI, 2.62-4.08), lack of split-dose bowel prep (OR, 2.67; 95% CI, 2.17-3.29), increased bowel prep-to-defecation interval (OR, 2.62; 95% CI, 1.53-4.50), nonadherence to dietary instructions (OR, 2.47; 95% CI, 1.94-3.14), increased prep-to-colonoscopy interval (OR, 2.29; 95% CI, 1.79-2.94), prep intolerance (OR, 2.14; 95% CI, 1.34-3.42), previous inadequate prep (OR, 2.11; 95% CI, 1.56-2.84) and inpatient status (OR, 1.74; 95% CI, 1.37-2.22).
The researchers concluded that these findings could help develop a model to identify patients at high risk for inadequate bowel prep and that future research should examine targeted interventions for patients with these risk factors.
Dr. Sharma is a member of the Gastroenterology & Endoscopy News editorial board.
This article is from the March 2025 print issue.