

VANCOUVER, B.C.—There is a long-standing belief that patients with a presumptive diagnosis of diverticulitis may instead be harboring colon cancer, but what is the real risk? In an analysis of a large database, patients whose diverticulitis is considered complicated—with abscess or perforation—had nearly a fourfold increased likelihood of having cancer or an advanced adenoma found on colonoscopy compared with the average-risk screening population. However, those with less severe diverticulitis had a decreased likelihood.
“Colon cancer can be misdiagnosed as diverticulitis, and for this reason colonoscopy is often recommended to exclude a missed cancer after patients recover from an episode of diverticulitis. However, this is a controversial recommendation that is based on limited evidence,” said investigator Walker D. Redd, MD, presenting the findings at the 2023 annual meeting of the American College of Gastroenterology (plenary 11). “Therefore, we felt that reliable estimates are needed to better understand whether this risk for colon cancer for the patient with diverticulitis is similar to or increased as compared to that of a screening population,” added Dr. Redd, a gastroenterology fellow at the University of North Carolina School of Medicine, in Chapel Hill.
GIQuIC Registry Explored
Dr. Redd and his co-investigators used the Gastrointestinal Quality Improvement Consortium (GIQuIC) endoscopy registry of patients treated at 779 U.S. sites to find patients aged 40 years and older who underwent outpatient colonoscopy for an indication of diverticulitis or average-risk screening between 2012 and 2021. The diverticulitis population was divided into four groups: patients with any diverticulitis, patients undergoing colonoscopy as a follow-up to a diverticulitis diagnosis, patients with uncomplicated diverticulitis and patients with complicated diverticulitis (i.e., abscess or perforation). The primary outcome was prevalence of adenocarcinoma on colonoscopy; prevalence of advanced neoplasia was the secondary outcome. Logistic regression adjusted for age, sex, race/ethnicity, ASA class, U.S. region, bowel prep, documentation of cecum and endoscopist adenoma detection rate.
The researchers identified 91,993 colonoscopies with a diverticulitis indication and 4,591,921 screening colonoscopies. For the reference number—the colonoscopy findings among the screening population—the prevalence of adenocarcinoma was 0.33% and the prevalence of advanced neoplasia was 6.9%.
Focus on Patients Who Have Complicated Diverticulitis
There was a low risk for adenocarcinoma or advanced neoplasia in most patients with diverticulitis, including those undergoing colonoscopy for diverticulitis follow-up, Dr. Redd said. However, patients with complicated diverticulitis had a nearly fourfold risk for adenocarcinoma, Dr. Redd reported (Table).
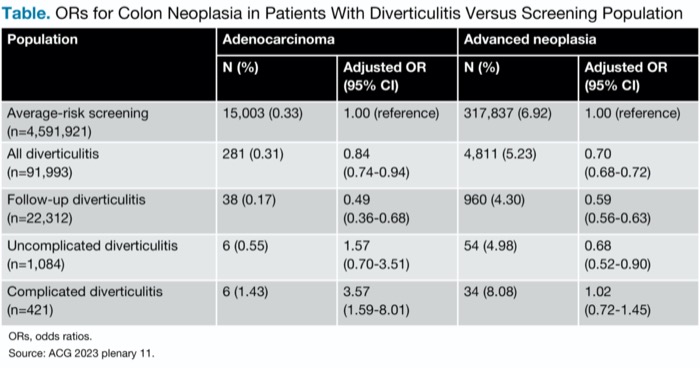
| Table. ORs for Colon Neoplasia in Patients With Diverticulitis Versus Screening Population | ||||
| Population | Adenocarcinoma | Advanced neoplasia | ||
|---|---|---|---|---|
| N (%) | Adjusted OR (95% CI) | N (%) | Adjusted OR (95% CI) | |
| Average-risk screening (n=4,591,921) | 15,003 (0.33) | 1.00 (reference) | 317,837 (6.92) | 1.00 (reference) |
| All diverticulitis (n=91,993) | 281 (0.31) | 0.84 (0.74-0.94) | 4,811 (5.23) | 0.70 (0.68-0.72) |
| Follow-up diverticulitis (n=22,312) | 38 (0.17) | 0.49 (0.36-0.68) | 960 (4.30) | 0.59 (0.56-0.63) |
| Uncomplicated diverticulitis (n=1,084) | 6 (0.55) | 1.57 (0.70-3.51) | 54 (4.98) | 0.68 (0.52-0.90) |
| Complicated diverticulitis (n=421) | 6 (1.43) | 3.57 (1.59-8.01) | 34 (8.08) | 1.02 (0.72-1.45) |
| ORs, odds ratios. Source: ACG 2023 plenary 11. | ||||
When the results were stratified by age, the risk for colon cancer increased with age, as expected. In patients with diverticulitis, the risks for cancer and advanced neoplasia remained similar to or below those of the screening population, he said.
“We think these findings have relevance to clinical practice. Some guidelines recommend colonoscopy for any patient with diverticulitis, whereas others recommend colonoscopy only for patients with complicated diverticulitis. Our findings suggest that for those with uncomplicated diverticulitis who do not have alarm symptoms, the recommendation to perform colonoscopy to exclude a missed cancer should be reconsidered, and, importantly, patients with complicated diverticulitis should undergo colonoscopy,” he concluded.
Session co-moderator Neil Stollman, MD, applauded the investigators for using the GIQuIC registry. “It’s a really good index for a test case like this,” said Dr. Stollman, the chief of the Division of Gastroenterology at Alta Bates Summit Medical Center, in Oakland, Calif., and an associate clinical professor of medicine at the University of California, San Francisco.
Dr. Stollman emphasized that the analysis did not include data on prior colonoscopies in this population. “Most of the recommendations for post-diverticulitis colonoscopy have a caveat: They say to do so ‘if a high-quality exam was not previously done’ within some recent time interval, although that interval is not precisely defined. I suspect that some or many of these patients have had a prior colonoscopy, which explains their actual lower risk.”
Although the lack of such information might be a limitation of the study, he added, the findings support the growing belief that it is the subset of patients with complicated diverticulitis who should be the “focus of our resources.”
—Caroline Helwick
Drs. Redd and Stollman reported no relevant financial disclosures.



This article is from the January 2024 print issue.