

PHOENIX—Use of a novel rigidizing overtube during colonic endoscopic submucosal dissection significantly improved scope stability and retroflexion and reduced reliance on adjunctive maneuvers, such as use of stiffeners and manual compression, in a study from Baylor College of Medicine, in Houston.
The study found procedural advantages that may enhance efficiency in selected cases and, importantly, showed the device, the GI Pathfinder (Neptune Medical), offers ergonomic benefits without compromising outcomes.
“It’s safer and more ergonomically friendly than conventional ESD. That, for me, as a female, is very important,” said Tara Keihanian, MD, MPH, describing to Gastroenterology & Endoscopy News how she and her female colleagues struggle with some aspects of the endoscopy equipment because of their small stature.
The GI Pathfinder was designed to manage loop formation, facilitate navigation to the target, and enhance control of the endoscopic tip (Figure). It originally was intended for use in upper endoscopy, but senior investigator Mohamed Othman, MD, a professor of medicine at Baylor and the chief of the gastroenterology and hepatology section, said he envisioned how its unique features would be valuable in ESD. He brought this to the attention of the manufacturer and thereafter consulted on the use of the GI Pathfinder for colonic endoscopic procedures.

About the Study
Presenting the single-center randomized controlled study, which earned several awards, at ACG 2025 (poster 1385), Dr. Keihanian reported that the investigators assessed the efficacy of the GI Pathfinder in 66 patients referred for resection of advanced polyps (granular lateral spreading tumors =3 cm or non-GLSTs =20 mm). They randomized patients to conventional ESD or overtube-assisted ESD performed by three endoscopists with varying levels of expertise. Exclusion criteria included polyps located in the ileocecal valve or appendix. The primary outcome was procedure speed; secondary outcomes included en bloc and R0 resection rates, dissection and closure speeds, and adverse events.
Multiple Advantages
The rigidizing overtube significantly improved scope stability and retroflexion capability and required less frequent use of a scope stiffener or manual abdominal pressure, the investigators reported (Table). In addition, a trend toward higher dissection speed with the overtube was observed, Dr. Keihanian reported.
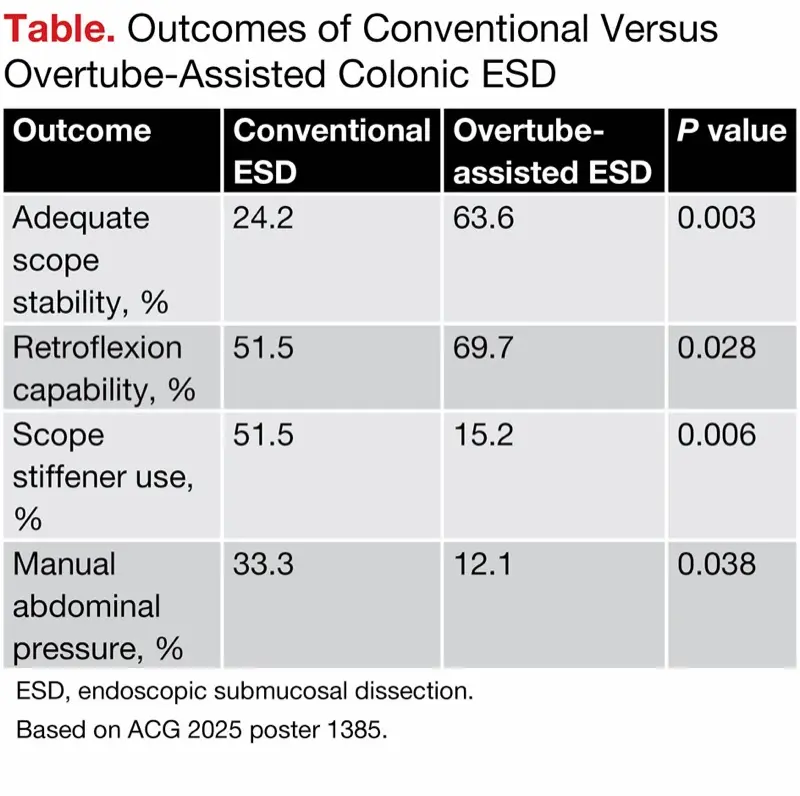
| Table. Outcomes of Conventional Versus Overtube-Assisted Colonic ESD | |||
| Outcome | Conventional ESD | Overtube- assisted ESD | P value |
|---|---|---|---|
| Adequate scope stability, % | 24.2 | 63.6 | 0.003 |
| Retroflexion capability, % | 51.5 | 69.7 | 0.028 |
| Scope stiffener use, % | 51.5 | 15.2 | 0.006 |
| Manual abdominal pressure, % | 33.3 | 12.1 | 0.038 |
| ESD, endoscopic submucosal dissection. Based on ACG 2025 poster 1385. | |||
En bloc and R0 resection rates were similar in the intention-to-treat analysis. Four patients crossed over from the control arm to the overtube arm (based on lack of achieving 1 cm2 per hour in 20 minutes), and three of these underwent completed en bloc resections. One crossed over from the overtube to the control arm and was resected piecemeal. Rates of intra- and postprocedural adverse events were comparable across both groups.
The overtube appears to overcome some of the challenges of performing ESD, especially in obese patients. Dr. Keihanian emphasized that “the tortuous and redundant anatomy of the colon can compromise the maneuverability and stability of the scope,” a challenge that is heightened by obesity.
“We can’t move obese patients, we can’t apply pressure, and often we ultimately can’t remove the polyp,” elaborated Dr. Othman. “The patient can end up with a right hemicolectomy, not because the lesion is cancer but because the scope is unstable.”
Dr. Keihanian described what, in her experience, has been the overtube’s main advantages in ESD: “I especially like how it works in retroflexion. It is completely stable. I can work within a particular view for whatever amount of time I need and it’s flexible. I can make it into any shape—a loop, a figure eight, whatever—and it will stay that way and not move.”
Device ‘Uniquely Positioned’
Mark Benson, MD, the section chief of advanced endoscopy at the University of Wisconsin School of Medicine and Public Health, in Madison, agreed that obese patients can present difficulties endoscopically. “Colonic ESD as well as complex EMR [endoscopic mucosal resection] can be challenging due to an unstable scope position for patients with long, redundant, tortuous colonic anatomy. Patients with significantly elevated BMIs [body mass indexes] can be uniquely difficult, as there are limitations to both abdominal pressure and patient position in this setting,” he told Gastroenterology & Endoscopy News.
“It is of paramount importance that the scope position is stable for complex EMR and ESD. Improved endoscopic control will improve patient safety as well as lead to a more thorough resection. A rigidizing overtube is uniquely positioned to improve endoscopic control and stability in specific clinical scenarios,” he said.
Dr. Benson added that he has not personally used the device evaluated in the study but said the results “convincingly added to the growing body of evidence supporting such overtubes for complex endoscopic procedures.” He said he anticipates more widespread use of these devices in the treatment of other disorders throughout the gastrointestinal tract.
—Caroline Helwick
Dr. Benson reported no relevant financial disclosures. Drs. Keihanian and Othman reported a financial relationship with Neptune Medical.



This article is from the February 2026 print issue.