

WASHINGTON—In a comparison of a standard liquid bowel preparation and tablet prep for colonoscopy among military personnel, tablets were preferred over liquid prep and there was little difference in cost to the healthcare system.
“This project demonstrates that, in multiple categories, tablet prep is preferred to liquid prep, with negligible cost differences,” said Christopher Casaccio, DO, who presented the poster at DDW 2024 (abstract Sa1122).
The study compared patient satisfaction and cost differential of tablet and liquid prep at a military treatment facility, Wright-Patterson Medical Center, in Dayton, Ohio.
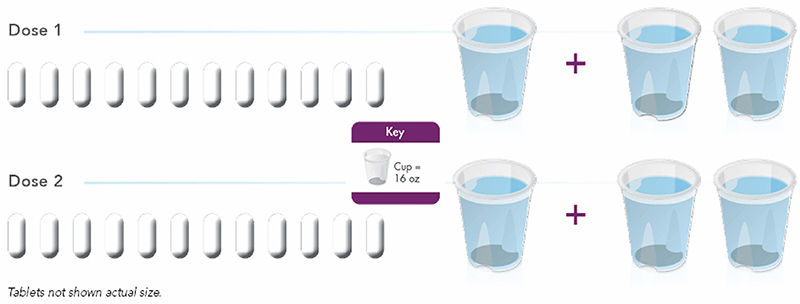
Investigators rotated the assignment of the prep between standard liquid prep with polyethylene glycol 3350, sodium sulfate, sodium chloride, potassium chloride, sodium ascorbate and ascorbic acid (Moviprep, Salix) and tablet prep with sodium sulfate, magnesium sulfate and potassium chloride (Sutab, Braintree/Sebela), which under the Department of Defense/TRICARE military healthcare system cost $15 and $68, respectively. Dr. Casaccio, a captain in the U.S. Air Force and an assistant professor at Wright State University Boonshoft School of Medicine, in Dayton, Ohio, acknowledged that these costs, which were negotiated, could be higher outside of the military. The investigators were able to estimate cost because of the DOD’s centralized healthcare system that covers nonvariable expenses, such as equipment and salaries, as well as variable expenses, such as patient medications and costs associated with services provided outside of the military treatment facility.
Tablets Preferred
Patients completed a survey to evaluate the ease and experience of receiving their assigned prep using a 5-point Likert scale and yes/no answers. The prep success rate was determined through a medical records review of colonoscopies and was found to be 97% and 94% for tablet and liquid preparations, respectively, although the number collected was not great enough to reach statistical significance.
In most categories, the tablet was preferred by patients (Table).
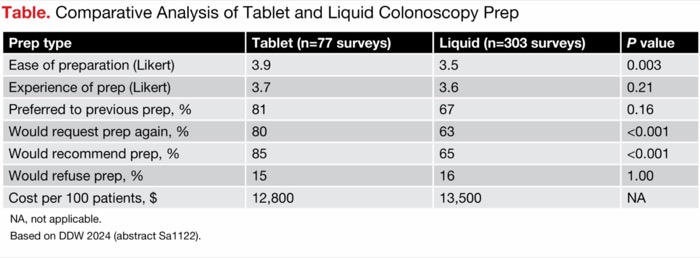
| Table. Comparative Analysis of Tablet and Liquid Colonoscopy Prep | |||
| Prep type | Tablet (n=77 surveys) | Liquid (n=303 surveys) | P value |
|---|---|---|---|
| Ease of preparation (Likert) | 3.9 | 3.5 | 0.003 |
| Experience of prep (Likert) | 3.7 | 3.6 | 0.21 |
| Preferred to previous prep, % | 81 | 67 | 0.16 |
| Would request prep again, % | 80 | 63 | <0.001 |
| Would recommend prep, % | 85 | 65 | <0.001 |
| Would refuse prep, % | 15 | 16 | 1.00 |
| Cost per 100 patients, $ | 12,800 | 13,500 | NA |
| NA, not applicable. Based on DDW 2024 (abstract Sa1122). | |||
The rate at which both groups said they would refuse the assigned prep for future exams was surprisingly low, Dr. Casaccio noted. “On most every data point, patients liked the tablet better. But we were hoping to see a difference in whether they would refuse the prep later, which would matter in terms of future compliance,” he said. As he pointed out, military personnel are generally compliant. “They are used to following orders. They typically do what their doctors ask.”
Potential for Cost Savings
Although the tablets as individual prescriptions were more than four times as expensive as the standard prep, tablet use overall helped the gastroenterology practice economically, Dr. Casaccio reported. “Our gastroenterologists run at full capacity. We lose money when a patient has a failed prep and has to reschedule. They take a spot and then we have to refer another patient off base. We pay that community gastroenterologist $2,000 to do that colonoscopy, instead of doing it ourselves.”



He acknowledged that outside of a structured payment system such as this, it would be more difficult to track costs, and that there may not be shared benefit of preventing preparation failures. He hopes that a large civilian system could re-create the project to estimate costs for the overall U.S. healthcare system.
Patients Should Know About Tablets
Brian C. Jacobson, MD, MPH, an associate professor of medicine at Harvard Medical School and the director of Program Development for Gastroenterology at Massachusetts General Hospital, in Boston, said he would like to see larger randomized trials showing at least comparable efficacy between tablets and liquid prep.
For now, until there are more reassuring data or inclusion in the guidelines, he said, “I tend to rely on the tried and true.” Nevertheless, he said he believes patients should be informed of this alternative to liquid prep. That is especially so for patients who tell him that they don’t want to drink “something that tastes putrid,” he said. He also noted that although the tablets cost more, “no patient has come back to me to complain.”
—Caroline Helwick
Drs. Casaccio and Jacobson reported no relevant financial disclosures. Disclaimer: The views and opinions expressed in this article are those of Dr. Casaccio and his co-investigators and do not necessarily reflect the official policy or position of the U.S. Air Force, Defense Health Agency, Department of Defense or U.S. government.
This article is from the January 2025 print issue.