


SAN DIEGO—A root cause analysis of data from a large Veterans Affairs healthcare system has revealed that most post-endoscopy gastric cancers can be attributed to missed precursor lesions on index esophagogastroduodenoscopy.
“Our analysis shows that missed opportunities account for 70% of post-endoscopy gastric cancer [PEGC]. This root cause analysis can standardize future investigations of post-endoscopy gastric cancer and guide implementation and adoption of quality indicators for esophagogastroduodenoscopy,” said Jenson Phung, MD, a third-year internal medicine resident at the University of Minnesota Twin Cities, in Minneapolis.
Dr. Phung noted that the five-year survival rate of only 36% for gastric cancer remains poor but potentially could be improved by early detection. “There is a growing body of evidence that gastric cancer can be missed and that patients are diagnosed with gastric cancer after a normal EGD in which no gastric cancer was detected. This potentially undermines the screening and diagnostic strategies for gastric cancer,” he said, reporting the findings at DDW 2025 (abstract 946).
To better understand the problem of PEGC, Dr. Phung and his co-investigators conducted a root cause analysis based on the “look-forward” methodology proposed by the World Endoscopy Organization for identifying post-colonoscopy colorectal cancers. The researchers retrospectively evaluated data from the VA Corporate Data Warehouse and central cancer registry for 2017 to 2021 to identify patients diagnosed with PEGC, which was defined as gastric adenocarcinoma occurring six to 36 months after an EGD in which no gastric cancer had been found. For the study, the most recent EGD prior to gastric adenocarcinoma diagnosis was considered the index EGD. More than 50% of index EGDs were done for alarm symptoms (anemia, weight loss, dysphagia, abnormal imaging).
Cases were first evaluated for the presence of a precursor lesion. Precursor lesions were defined via the presence of atrophic gastritis, gastric intestinal metaplasia, adenomas or positive Helicobacter pylori on index EGD. Adequate endoscopy and follow-up were determined by written or photo documentation of a complete exam and adherence to the American Gastroenterological Association guidelines on follow-up.
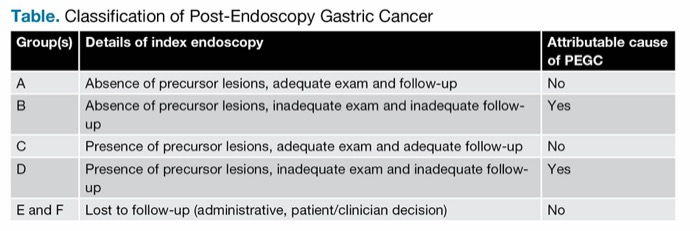
PEGC cases were divided into the five categories shown in the Table. An adequate exam and follow-up was not considered an attributable cause of missed cancer (groups A and C), but an inadequate index endoscopy and follow-up was (groups B and D). Missed cancer also was not attributed to the index colonoscopy in those lost to follow-up (groups E and F). The primary outcome was the proportion of PEGC cases deemed attributable to a missed gastric cancer on index EGD.
| Table. Classification of Post-Endoscopy Gastric Cancer | ||
| Group(s) | Details of index endoscopy | Attributable cause of PEGC |
|---|---|---|
| A | Absence of precursor lesions, adequate exam and follow-up | No |
| B | Absence of precursor lesions, inadequate exam and inadequate follow-up | Yes |
| C | Presence of precursor lesions, adequate exam and adequate follow-up | No |
| D | Presence of precursor lesions, inadequate exam and inadequate follow-up | Yes |
| E and F | Lost to follow-up (administrative, patient/clinician decision) | No |
Precursor Lesions in One-Third Of Patients
Seventy-six patients met the criteria for PEGC in this root cause analysis: 96% were male, median age was 70 years, and the median time between the index EGD and PEGC diagnosis was 18 months. The most common sites of PEGC were the antrum (19.7%) and the body (19.7%).
Among these patients, 32.9% had precursor lesions on index EGD. Groups B and D included 34 and 19 patients, respectively, constituting a total of 53 PEGC cases deemed attributable to a missed cancer on the index EGD (69.7%). The remaining cases in which PEGC was not attributable to a missed cancer on the index EGD were: group A, 18.4%; group C, 3.95%; group E, 3.95%; and group F, 3.95%.
For the 53 cases deemed attributable to a missed cancer on the index exam, 48 (63.2%) were determined to have had an inadequate index EGD and 19 (25.0%) were believed to have had inadequate follow-up. In 14 patients (18.4%), both the examination and follow-up were deemed inadequate, Dr. Phung reported.
There were 69 deaths among these patients, 50 (72.5%) of which were related to PEGC. More than half the patients (52%) had metastatic disease at the time of PEGC diagnosis.
“We found we had a similar rate of attributable cases, about two-thirds of patients, as suggested by existing data from a root cause analysis performed for all upper GI cancers from 2023 [Endoscopy 2023;55(2):109-118],” Dr. Phung said.
“Our findings emphasize areas for improvement in the optical detection and diagnosis of gastric precursor lesions,” he said. “It also highlights “the need for implementation of upper GI endoscopy quality metrics, [as well as] improvements in institutional pathways and [a] framework to standardize endoscopic exams.”
‘Optimizing Visual and Diagnostic Parameters’
Related Content



Rashmi Advani, MD, an assistant professor of medicine at Icahn School of Medicine at Mount Sinai, in New York City, and the director of bariatric endoscopy at the Center for Interventional Endoscopy at Mount Sinai South Nassau, in Bellmore, N.Y., told Gastroenterology & Endoscopy News that the study is “a very thorough review” of the problem of PEGC. However, its impact is limited by its retrospective nature, she said, since large-scale randomized trials are necessary to establish the true degree to which precursor gastric lesions are missed endoscopically.
However, the study should be the starting point of a conversation about a new direction toward “optimizing our visual and diagnostic parameters when performing endoscopy,” Dr. Advani emphasized. “This also may include the implementation of artificial intelligence as an adjunctive tool to help characterize areas of the stomach that may harbor a precursor lesion but are not obvious to the eye of the endoscopist. It also may set the stage for the development of better endoscopes, with features for improving optical resolution.
“More robust patient follow-up protocols may also need to be instilled on a standardized scale to ensure proper endoscopic management, should precursor conditions lead to high-risk lesions in the stomach that can ultimately become gastric cancer,” she added. “Lastly, it may influence large health systems, including the VA, to invest in these newer technologies to optimize early diagnosis and, thus, treatment of gastric cancer.”
—Caroline Helwick
Dr. Advani reported financial relationships with Boston Scientific and Medtronic. Dr. Phung reported no relevant financial disclosures.
This article is from the August 2025 print issue.