

Busy endoscopists perform hundreds of procedures annually, and unfortunately, this takes a toll. A meta-analysis found nearly 58% of endoscopists reported a work-related injury, with the most common sites of injury being the hands, fingers, back and neck (Gastrointest Endosc 2023;98[4]:482-491).
Efforts to address this problem have grown over the last several years, with the American Gastroenterological Association, American College of Gastroenterology and American Society for Gastrointestinal Endoscopy providing a multitude of resources, and manufacturers working to develop scopes that accommodate different-sized endoscopists. More awareness and change are required, experts say.
“It’s a one-size-fits-all device for a not-one-sized workforce,” said Swati Pawa, MD, a professor at Wake Forest University, in Winson Salem, N.C. and lead author of the ASGE guideline. “There haven’t yet been significant advances in endoscope design.”
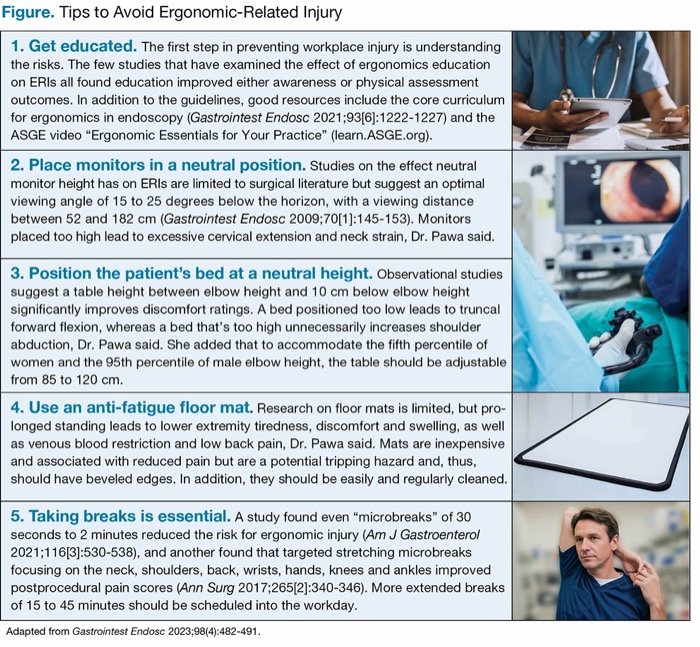
| Figure. Tips to Avoid Ergonomic-Related Injury | |
| 1. Get educated. The first step in preventing workplace injury is understanding the risks. The few studies that have examined the effect of ergonomics education on ERIs all found education improved either awareness or physical assessment outcomes. In addition to the guidelines, good resources include the core curriculum for ergonomics in endoscopy (Gastrointest Endosc 2021;93[6]:1222-1227) and the ASGE video “Ergonomic Essentials for Your Practice” (learn.ASGE.org). | |
| 2. Place monitors in a neutral position. Studies on the effect neutral monitor height has on ERIs are limited to surgical literature but suggest an optimal viewing angle of 15 to 25 degrees below the horizon, with a viewing distance between 52 and 182 cm (Gastrointest Endosc 2009;70[1]:145-153). Monitors placed too high lead to excessive cervical extension and neck strain, Dr. Pawa said. | |
| 3. Position the patient’s bed at a neutral height. Observational studies suggest a table height between elbow height and 10 cm below elbow height significantly improves discomfort ratings. A bed positioned too low leads to truncal forward flexion, whereas a bed that’s too high unnecessarily increases shoulder abduction, Dr. Pawa said. She added that to accommodate the fifth percentile of women and the 95th percentile of male elbow height, the table should be adjustable from 85 to 120 cm. | |
| 4. Use an anti-fatigue floor mat. Research on floor mats is limited, but prolonged standing leads to lower extremity tiredness, discomfort and swelling, as well as venous blood restriction and low back pain, Dr. Pawa said. Mats are inexpensive and associated with reduced pain but are a potential tripping hazard and, thus, should have beveled edges. In addition, they should be easily and regularly cleaned. | |
| 5. Taking breaks is essential. A study found even “microbreaks” of 30 seconds to 2 minutes reduced the risk for ergonomic injury (Am J Gastroenterol 2021;116[3]:530-538), and another found that targeted stretching microbreaks focusing on the neck, shoulders, back, wrists, hands, knees and ankles improved postprocedural pain scores (Ann Surg 2017;265[2]:340-346). More extended breaks of 15 to 45 minutes should be scheduled into the workday. | |
| Adapted from Gastrointest Endosc 2023;98(4):482-491. | |
A 2022 study found endoscopists with smaller hand size had better baseline dexterity measures but performed procedures more slowly and reported more fatigue than those with larger hands (Am J Surg 2023;225[2]:378-382). No differences in procedure time or fatigue were observed between hand sizes when using a bronchoscope.
While institutional-level innovation is likely beyond an endoscopist’s control, here are some practical, easy tips from the ASGE guideline that can reduce the chance of an ergonomic-related injury (Gastrointest Endosc 2023;98[4]:482-491).
—Katie Prince
 Check out more on ergonomics for nurses and support staff in “Highlights of SGNA 2025: Nurse Training, Ergonomics, GLP-1 Safety, and More.” Cynthia Friis, MEd, BSN, RN, discusses an abstract on an ergonomics initiative that improved satisfaction and comfort in the endoscopy unit.
Check out more on ergonomics for nurses and support staff in “Highlights of SGNA 2025: Nurse Training, Ergonomics, GLP-1 Safety, and More.” Cynthia Friis, MEd, BSN, RN, discusses an abstract on an ergonomics initiative that improved satisfaction and comfort in the endoscopy unit.This article is from the October 2025 print issue.