


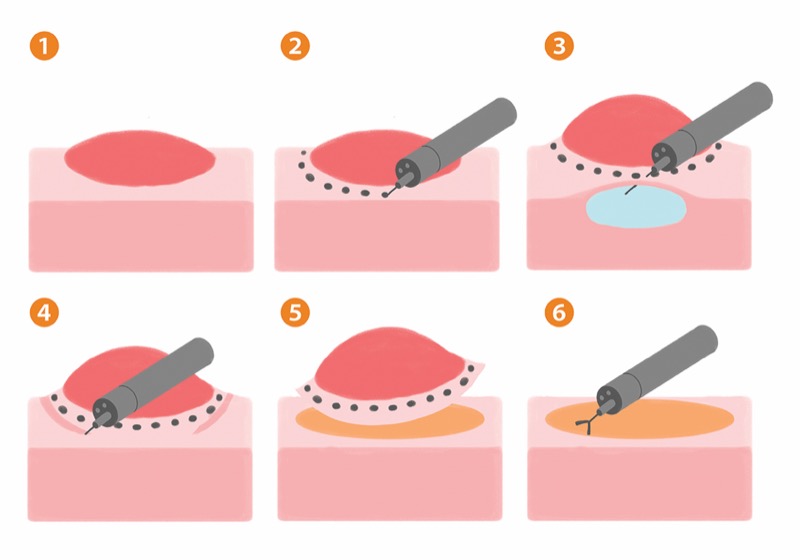
SAN DIEGO—A large matched propensity analysis found that endoscopic submucosal dissection is a safe and effective salvage treatment for residual colorectal polyps after failed endoscopic resection, according to study results presented at DDW 2025.
“We can conclude that ESD is a viable and safe rescue technique for managing large nonpedunculated colorectal polyps after failed endoscopic resection, with outcomes aligning with established quality benchmarks,” said Ernesto Robalino Gonzaga, MD, an assistant professor of clinical medicine at the University of Pennsylvania Perelman School of Medicine, in Philadelphia. Dr. Gonzaga led the research during his fellowship at AdventHealth Medical Group in Orlando, Fla.
Current guidelines from the U.S. Multi-Society Task Force on Colorectal Cancer suggest that ESD can be an effective salvage treatment option after failed endoscopic mucosal resection (EMR), but experience in this setting remains limited in the West (Am J Gastroenterol 2020;115[3]:435-464). Dr. Gonzaga and his co-investigators evaluated this approach in patients with previously attempted incomplete EMR, comparing outcomes in this group with those in treatment-naive patients undergoing ESD of large nonpedunculated colorectal polyps.
To do this, they conducted a multicenter matched propensity analysis of 1,447 patients treated by advanced endoscopists (at least three years of experience with ESD) at 11 medical centers over a three-year period (abstract 859). The researchers accounted for age, sex, lesion size and location, morphology, histology, and degree of fibrosis, ultimately matching 361 treatment-naive patients with 184 failed-EMR patients for the 2-to-1 propensity score analysis.
There were no statistically significant differences between the two comparison groups in terms of patient or lesion characteristics. Mean lesion size was approximately 34 mm; most were laterally spreading granular adenomas/serrated adenomas in the right colon.
The degree of submucosal fibrosis was similar between the groups—approximately 68% in the failed-EMR group and 63% in treatment-naive patients—but prior manipulation of the lesions differed in that tattoos were visible in 15.2% of failed EMR and 26.6% of treatment-naive cases, and biopsies had been taken on 9.8% and 60.1% of failed EMR and treatment-naive cases, respectively.
Results of ESD After Failed EMR
Dr. Gonzaga reported no differences between the treatment-naive and failed EMR groups in resection rates after ESD (Table). However, median procedure times were longer in the treatment-naive group (94 minutes) than in the failed-EMR group (85 minutes; P=0.01).
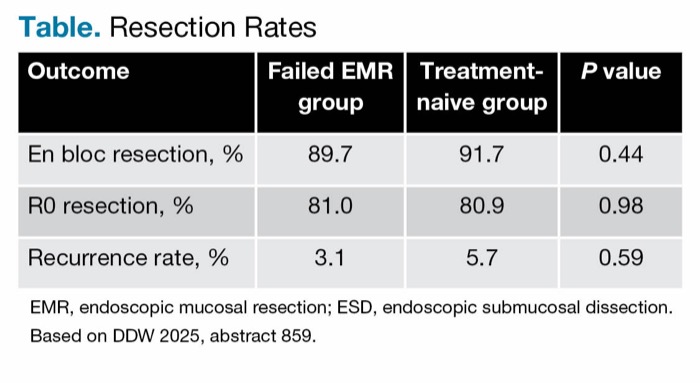
| Table. Resection Rates | |||
| Outcome | Failed EMR group | Treatment-naive group | P value |
|---|---|---|---|
| En bloc resection, % | 89.7 | 91.7 | 0.44 |
| R0 resection, % | 81.0 | 80.9 | 0.98 |
| Recurrence rate, % | 3.1 | 5.7 | 0.59 |
| EMR, endoscopic mucosal resection; ESD, endoscopic submucosal dissection. Based on DDW 2025, abstract 859. | |||
The investigators speculated that, while still very low, the numerically higher recurrence rate for the treatment-naive control arm may reflect procedures that were performed earlier in the learning curve of ESD. They also are exploring whether expertise among centers varies depending on caseload.
Adverse event rates were low overall. Perforation rates were almost identical, 4.3% in the failed-EMR group and 4.7% in the treatment-naive group. Although delayed bleeding was twice as common in the failed-EMR group (1.6% vs. 0.8%), this trend did not reach statistical significance (P=0.41), Dr. Gonzaga reported.
“All bleeding episodes were managed endoscopically—only 0.5% needed interventional radiology involvement,” he said. “Most of the perforations were treated with endoscopy. Only two patients from the failed-endoscopy group were treated with surgery, likely because of the presence of fibrosis which, as we know, is one of the strongest risk factors for perforation.”
Because of the slight numerical increase in bleeding risk, the authors emphasized that salvage ESD should be considered an alternative to surgery only in centers with appropriate expertise. The researchers said they hope prospective studies will validate their findings and refine patient criteria so this minimally invasive salvage treatment option can reach more patients.
Michael Bourke, MD, the director of gastrointestinal endoscopy at Westmead Hospital, in New South Wales, Australia, who has pioneered considerable research in EMR and ESD for colorectal polyps, congratulated the authors for their “nice work,” but said a limitation of the study was its lack of a satisfying definition of endoscopy resection failure.
“I think it’s critical to define what failed endoscopic resection is. … For example, is it a polyp that is half resected? The polyps in this study could have barely been treated if their mean size was still 34 mm. … We need to know what patients you are comparing,” he suggested. “You have to define this very carefully, then stratify patients within that group by exactly what that failure was.”
—Caroline Helwick
Drs. Bourke and Gonzaga reported no relevant financial disclosures.



This article is from the October 2025 print issue.