

WASHINGTON—Can you identify patients in your practice with a high risk for inadequate bowel preparation before colonoscopy? When you do, how do you address the problem?
At DDW 2024, Brian C. Jacobson, MD, MPH, an associate professor of medicine at Harvard Medical School and the director of program development for gastroenterology at Massachusetts General Hospital, in Boston, provided some tips gastroenterologists can use to help patients optimize their prep.

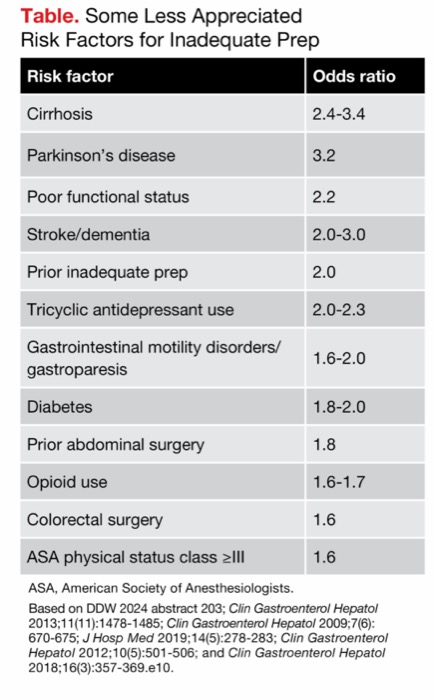
As Dr. Jacobson noted, some risk factors for inadequate prep are well established: age over 65 years, male sex, body mass index more than 30 kg/m2, a lower level of education, inpatient status, Medicare or Medicaid instead of private insurance, hypertension, tobacco use, and constipation. However, he said the published odds ratios (ORs) for these factors are fairly low—1.5 or under—and “some of the other risk factors for poor bowel prep may surprise you.” He said these less appreciated risk factors actually carry a higher risk (Table).
| Table. Some Less Appreciated Risk Factors for Inadequate Prep | |
| Risk factor | Odds ratio |
|---|---|
| Cirrhosis | 2.4-3.4 |
| Parkinson’s disease | 3.2 |
| Poor functional status | 2.2 |
| Stroke/dementia | 2.0-3.0 |
| Prior inadequate prep | 2.0 |
| Tricyclic antidepressant use | 2.0-2.3 |
| Gastrointestinal motility disorders/gastroparesis | 1.6-2.0 |
| Diabetes | 1.8-2.0 |
| Prior abdominal surgery | 1.8 |
| Opioid use | 1.6-1.7 |
| Colorectal surgery | 1.6 |
| ASA physical status class =III | 1.6 |
| ASA, American Society of Anesthesiologists. Based on DDW 2024 abstract 203; Clin Gastroenterol Hepatol 2013;11(11):1478-1485; Clin Gastroenterol Hepatol 2009;7(6): 670-675; J Hosp Med 2019;14(5):278-283; Clin Gastroenterol Hepatol 2012;10(5):501-506; and Clin Gastroenterol Hepatol 2018;16(3):357-369.e10. | |
As single characteristics, these risk factors are not particularly predictive, but in combination, their risk is cumulative. In a study of 1,588 outpatient colonoscopies, risk increased linearly according to number of risk factors, plateauing at a 98% likelihood of an inadequate bowel preparation when seven factors were present (Clin Gastroenterol Hepatol 2009;7[6]:670-675).
How to Address the High-Risk Group
Related Content



Once high-risk patients have been identified, what is the best way to reduce the likelihood of a poor prep? Navigation has been established as helpful “in getting patients over the finish line” with an adequate bowel prep, Dr. Jacobson said. “You might offer additional navigation, enhanced instructions, videos and so forth,” he suggested. While ideally all patients in one’s practice might benefit from a more intensive approach, “if you lack the resources, you could focus on the high-risk patients,” he said.
Modification of the bowel prep is another approach. A single-center randomized trial of 256 adults with previous inadequate prep evaluated two intensive regimens: a 4-L, split-dose polyethylene glycol (PEG) regimen versus 2-L, split-dose PEG plus ascorbic acid (Am J Gastroenterol 2017;112[6]:951-958). All participants underwent a three-day low-residue diet and received 10 mg of bisacodyl the day before colonoscopy. Adequate bowel cleansing by the Boston Bowel Preparation Scale (BBPS) was significantly more likely in patients assigned to the 4-L PEG regimen: 81.1% versus 67.4% (OR, 2.07) by intention-to-treat analysis and 86.6% versus 71.71% (OR, 2.55) by per-protocol analysis. However, Dr. Jacobson noted that although the “traditional” 4-L PEG approach was superior, the adequacy rate was still only 81% in this group of patients with a previous poor prep.
A similar multicenter Canadian study showed a 4-L, split-dose prep to be as effective as a 6-L prep in patients who received 15 mg of bisacodyl the day before colonoscopy plus several days of a low-fiber diet followed by a clear liquid diet the day before the exam (Clin Gastroenterol Hepatol 2022;20[6]:e1283-e1291). Patients in the lower volume group also expressed more willingness to repeat the prep.
“It’s not just the prep you choose. It’s also the timing—when they drink it, when they stop it,” he added. “If any of these things breaks down, the prep quality may not be adequate.”
Although European and U.S. guidelines have moved toward including low-residue/low-fiber diets in their recommendations, Dr. Jacobson said he still advocates the “non–patient-centered approach” of clear liquids the day before, “if patients are OK with it.”
State-of-the-Art Bowel Prep Process
Dr. Jacobson offered the following components for the bowel prep process:
- verbal and written instructions for all the components of a colonoscopy prep;
- some form of patient navigation; this can include telephonic or virtual navigation employing automated electronic messaging;
- low-residue/low-fiber or full liquid diet the day before colonoscopy;
- split-dose and 2-L bowel prep regimens instead of 4-L regimens;
- same-day regimen for afternoon colonoscopy, if desired;
- second half of split-dose regimen given four to six hours before colonoscopy, finished at least two hours prior to start;
- simethicone as the only adjunct to consider, taken as part of prep to reduce bubbles in the colon and improve visualization (although probably not covered by insurance); and
- use of an irrigation pump during colonoscopy.
“Remember that instructions should be language-congruent. If your patient is not a native English speaker, an eight-page booklet written entirely in English may not be the patient-centered approach you want to take,” he added.
New Frontier: Digital Solutions
The patient’s self-report of bowel prep adequacy usually is not reliable, showing about a 50% correlation with the actual prep quality. Artificial intelligence might be helpful not only in identifying patients at higher risk but also in helping them achieve adequate bowel preparation.
“I think we will start seeing AI platforms that can dig into the patient’s electronic health record, look at their diagnostic codes and medications, determine who is at high risk for a bad prep and flag this,” Dr. Jacobson predicted. “Schedulers can then act accordingly, and we can offer them personalized preps.”
The ability to help patients assess their own bowel prep quality was shown in a 2022 study of 1,434 patients in China (Am J Gastroenterol 2022;117[9]:1437-1443). Investigators developed an AI platform that used a convolutional neural network model (AI-CNN model) to evaluate the quality of prep in real time before colonoscopy; the control arm was visual assessment, and the result was pass or not pass. In the AI-CNN arm, patients downloaded a program to their smartphones into which they entered photos of toilet contents and received feedback and further instructions from the program.
Significant differences were not observed between the two groups in terms of mean BBPS scores (91% in each arm), polyp detection rate and adenoma detection rate. But in an analysis restricted to the patients with pass results, the AI-CNN–guided patients achieved higher mean BPPS scores. Although the AI-CNN program was not particularly more effective in this study, Dr. Jacobson said, “in principle, it’s interesting and rather exciting.”
Dr. Jacobson reported no relevant financial disclosures.
This article is from the November 2024 print issue.