

Once a year, Kathryn Felts, BSN, completes training on radiation safety required by The University of Texas MD Anderson Medical Center, in Houston, where she has worked for 12 years. However, data suggest many of her peers do not receive this education, and no national education standards exist.
“There’s a huge difference between the radiation safety here at MD Anderson and what we had at the hospital that I came from,” Ms. Felts said. “I think [education] helps us understand how to best protect ourselves, understand our risk, and do the right things in procedures to protect patients as well.”
Even endoscopists rarely receive adequate education on the risks and appropriate protocols around fluoroscopy used in endoscopic retrograde cholangiopancreatography and other GI procedures, said Meera Bhardwaj, MD.
Dr. Bhardwaj explained that medical radiation comprises about half of radiation exposure in the United States, and its use in healthcare is guided by the “as low as reasonably achievable,” or ALARA, principle for radiation safety. A list of international and national recommended thresholds is shown in Table 1.
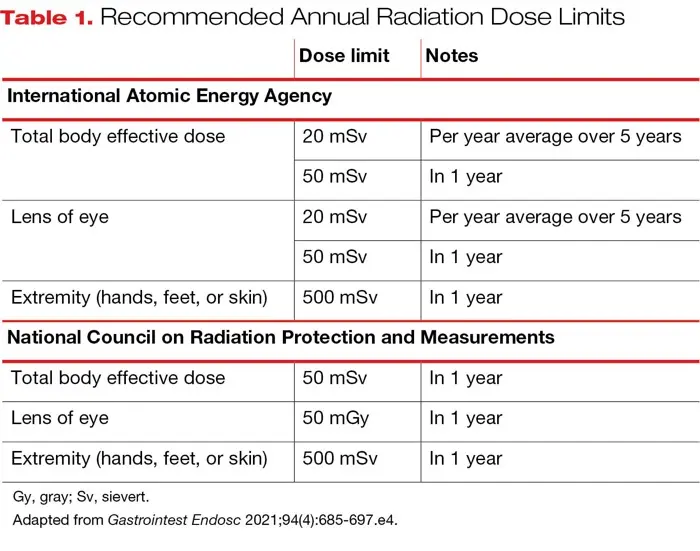
| Table 1. Recommended Annual Radiation Dose Limits | ||
| Dose limit | Notes | |
|---|---|---|
| International Atomic Energy Agency | ||
| Total body effective dose | 20 mSv | Per year average over 5 years |
| 50 mSv | In 1 year | |
| Lens of eye | 20 mSv | Per year average over 5 years |
| 50 mSv | In 1 year | |
| Extremity (hands, feet, or skin) | 500 mSv | In 1 year |
| National Council on Radiation Protection and Measurements | ||
| Total body effective dose | 50 mSv | In 1 year |
| Lens of eye | 50 mGy | In 1 year |
| Extremity (hands, feet, or skin) | 500 mSv | In 1 year |
| Gy, gray; Sv, sievert. Adapted from Gastrointest Endosc 2021;94(4):685-697.e4. | ||
According to the American Society of Radiologic Technologists, only eight states—Alaska, California, Colorado, Maryland, Nebraska, Nevada, New Jersey, and Texas—have any licensure or education standard requirement for fluoroscopy use, and no federal standard exists. However, training interventions have the potential to significantly improve staff knowledge and comfort level, said Dr. Bhardwaj, an interventional gastroenterologist and assistant professor of medicine at Stony Brook University Hospital, in New York.
Dr. Bhardwaj called for radiation education to become standard in fellowship programs, citing a 2019 study by researchers at Stanford University, in California, that found that approximately 55% of attending gastroenterologists and 79% of fellows had received no training in the use of their institution’s fluoroscopy equipment (Dig Dis Sci 2019;64[9]:2455-2466).

Monique Barakat, MD, an assistant professor of gastroenterology at Stanford, who co-authored the 2019 paper Dr. Bhardwaj referenced, told GEN Priority Report that the dearth of education in endoscopy is part of what prompted her and her co-investigators to gather real-world data on the topic.
“There’s not an emphasis on standards, education, just making sure people know the risks,” Dr. Barakat said. “It’s possible to perform these procedures safely with the right mentality to minimize radiation exposure, with the right approach to protection, but if people aren’t aware of the protection options, if they’re not aware of the minimization strategies, it’s tough.”
3 Pillars of ALARA
Time, distance, and shielding are the pillars of ALARA, Dr. Bhardwaj noted, outlining strategies endoscopy staff should employ to mitigate their exposure and maximize their safety.
Exposure Time
To help limit radiation exposure time during an ERCP, Dr. Bhardwaj said, use a pulsed rather than continuous image (Table 2). “You may have a little bit more radiation to produce that (pulse) image, but overall, you’re shooting the beam less, and that may, ultimately, result in less radiation exposure with a pulse image compared to continuous.”
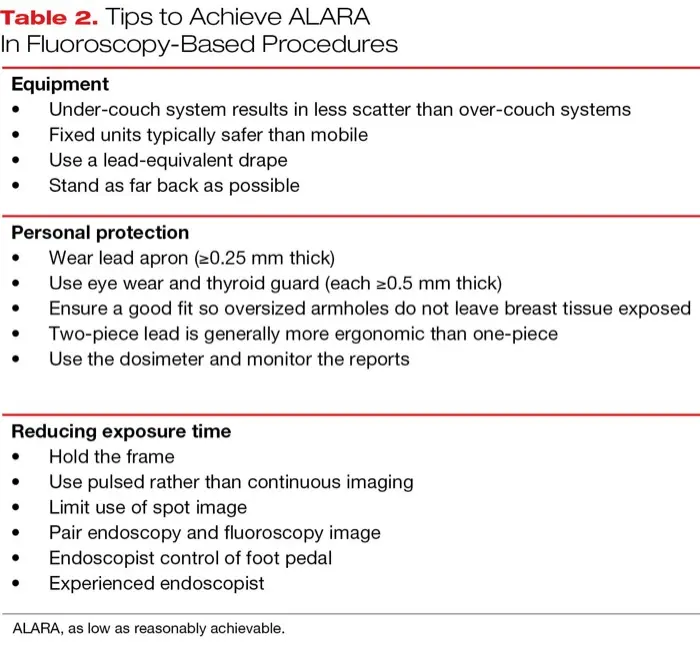
| Table 2. Tips to Achieve ALARA In Fluoroscopy-Based Procedures |
|
|
|
| ALARA, as low as reasonably achievable. |
Also, the hold frame function available on most newer units keeps an image on the screen for closer examination and discussion without using fluoroscopy, she said. “If that image wasn’t on the monitor, you’d have to hit the fluoro pedal and you have continuous radiation during those moments,” she explained, adding that the hold function has been shown to decrease radiation by 50% to 80%.
Another way to minimize radiation exposure is to ensure the endoscopy and fluoroscopy monitors are side by side, Dr. Bhardwaj said. When the endoscopists and the tech can work together, she said, that results in an average of 1.4 minutes less fluoroscopy time.
Dr. Bhardwaj cited a study that found that every 10 years of independent practice was associated with a 21% decrease in fluoroscopy time. The 2019 Stanford study, which found approximately 40% of fluoroscopy equipment was operated by radiology technicians, also underscored the importance of endoscopist-directed fluoroscopy, citing a 2018 study that found proceduralist-driven ERCP resulted in a 43% average reduction in radiation time and a 60% decrease in total radiation dose (Gastrointest Endosc 87[6 suppl 1]:AB48).
“I think at this hospital, we are pretty aware, but I believe that’s because our hospital and radiology staff are committed to keeping us educated,” Ms. Felts said. “The teaching/attending MDs take responsibility to teach the fellows regarding minimal use of the foot pedal during procedures to limit exposure to patient and staff.”
Keep a Safe Distance
Another key factor to consider is distance, Dr. Bhardwaj said, noting that most scatter comes from the patient. Larger patients mean more scatter, she noted, and radiation exposure is inversely proportional to the distance from the source, advising staff not directly involved in the procedure to stand as far back as possible.
Wear Protection
Most studies on radiation safety have indicated that nearly all endoscopy staff should wear a lead apron, including Dr. Barakat’s Stanford study, but the same data showed that more than one-fourth of participants reported they rarely or never wore a radiation dosimeter.
Dr. Bhardwaj noted that a lead apron alone is insufficient to ensure optimal protection. Lead comes in three thicknesses, and the lowest, 0.25 mm, blocks 90% of scatter, without the heaviness of the 0.5- and 1-mm options. A good fit is essential, she said, and two-piece lead usually is more ergonomic. She noted that lead should be hung rather than folded to prevent cracking, and it should be inspected annually. She also recommended a thyroid shield and 0.5-mm-thick eye protection.
Regular inspection of the lead gowns, along with instructions on how to prevent damage to their protective properties, is protocol at MD Anderson, Ms. Felts said, adding that the physicians can order custom-fit lead and goggles and are very concerned about protection. However, she said she was never provided thyroid shields at her previous workplace, despite the many years that she “stood next to the C-arm assisting with the ERCP procedures.”
Both Drs. Bhardwaj and Barakat said they are not sure why radiation safety does not receive more emphasis in fellowship programs or from national GI organizations, but each said she has seen firsthand that even brief instruction can significantly reduce exposure.
“Education does help,” Dr. Bhardwaj said. “I think that’s the key moving forward for mitigating risks for physicians and staff during these cases.”
Institutions bear some responsibility in ensuring their staff and patients are well protected, Ms. Felts said. “Since the facilities will have to make financial decisions about how to spend their money, such as fluoroscopy [equipment] and care, maintenance, and replacement of gowns and thyroid shields, … [they] should be held accountable, with the radiology department setting the standard of protection and ensuring those standards are consistent throughout the facility.”
—Katie Prince
Drs. Barakat and Bhardwaj and Ms. Felts reported no relevant financial disclosures.
This article is from the December 2025 Priority Report print issue.